Congenital heart disease (ASD – OS): A case report
Devi1, Sheetal2
Staff Nurse, Kauvery Hospital, Tirunelveli
Nursing Incharge, Kauvery Hospital, Tirunelveli
Abstract
Atrial septal defect (ASD) is one of the most common types of congenital heart defects, occurring in about 25% of children. An atrial septal defect occurs when there is a failure to close the communication between the right and left atria. It encompasses defects involving both the true septal membrane and other defects that allow for communication between both atria. There are five types of atrial septal defects ranging from most frequent to least: patent foramen ovale, ostium secundum defect, ostium primum defect, sinus venosus defect, and coronary sinus defect. Small atrial septal defects usually spontaneously close in childhood. Large defects that do not close spontaneously may require percutaneous or surgical intervention to prevent further complications such as stroke, dysrhythmias, and pulmonary hypertension.
This activity describes the evaluation, diagnosis, and management of a patient with atrial septal defect and highlights the role of team-based interprofessional care for affected patients.
Background
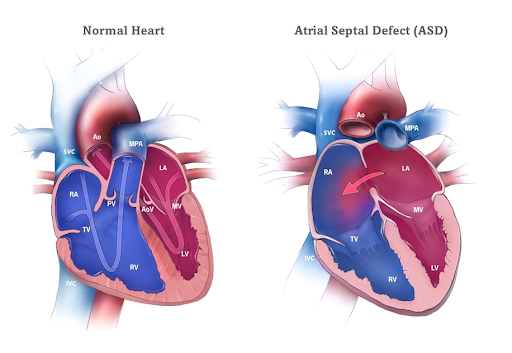
An ostium secundum atrial septal defect is a type of congenital heart defect called an atrial septal defect (ASD). This is the most common type of ASD, (80% of all ASDs).
An ASD is a hole in the wall (septum) between the two upper chambers of the heart (the atria). ASDs can be classified by location. An ostium secundum ASD is a hole in the center of the atrial septum. Normally, the right side of the heart pumps oxygen-poor blood to the lungs, while the left side pumps oxygen-rich blood to the body. An ASD allows blood from both sides to mix, causing the heart to work less efficiently.
A small hole may not cause any symptoms or problems. A larger hole can eventually cause symptoms such as shortness of breath, respiratory infections, fainting, irregular heart rhythms or fatigue after mild activity. Larger ASDs can also ultimately lead to pulmonary artery hypertension, right ventricular hypertrophy (enlargement); SVT, or heart failure.
Case Presentation
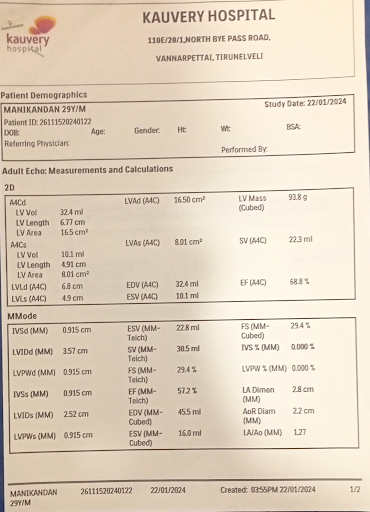
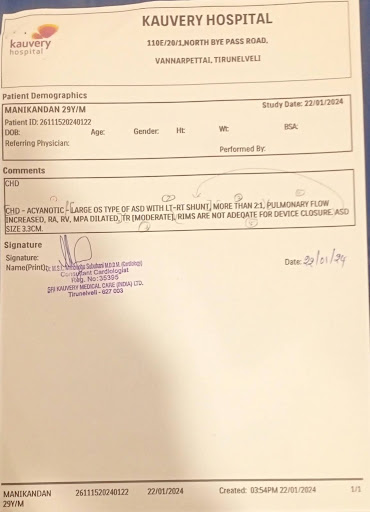
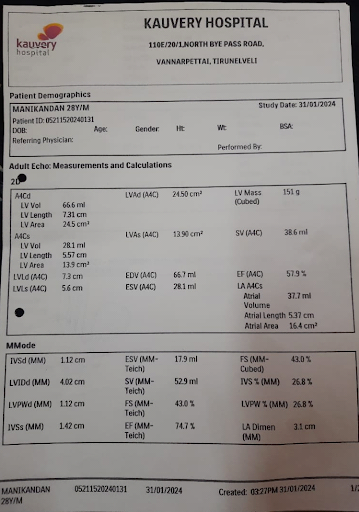
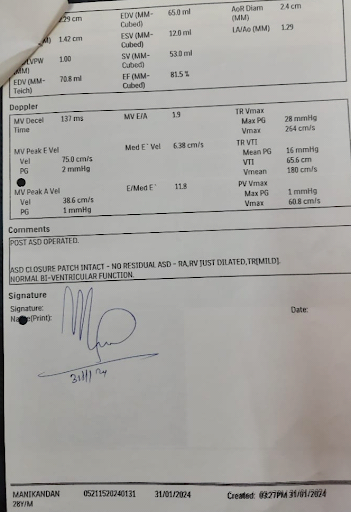
A 28 years old male presented with abrupt onset dyspnea and cough of three-month duration. Chest x ray reported cardiomegaly. Echocardiography identified a 3.3cm ostium secundum atrial septal defect with pulmonary hypertension, moderate tricuspid regurgitation (TR). This report emphasizes the importance of educating patients about congenital malformations and advising surgical correction.
On Clinical Assessment
BP: 110/70 mm/hg,
HR: 76b/mts,
Resp: 16b/mts,
Tem: 98.6f,
SPo2: 99%
Auscultation
Systolic murmur
Right heart enlargement.
Abnormal heart rhythm.
Pulmonary hypertension.
Investigation
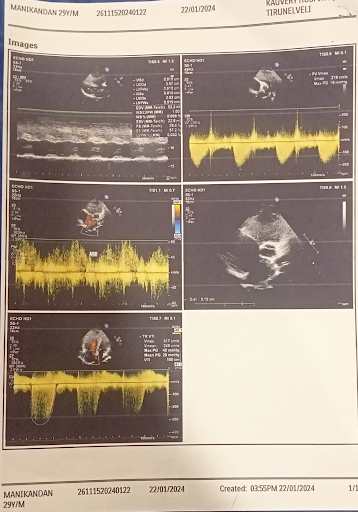
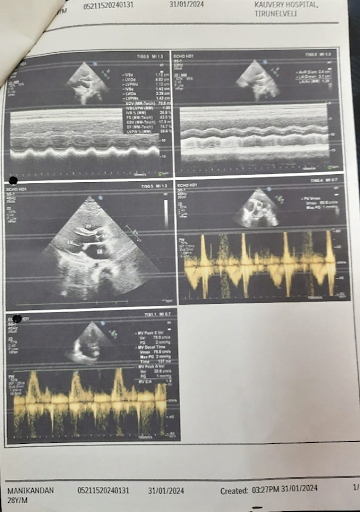
1. ECHO,
2. D and Doppler studies: Osteum Secondum, ASD
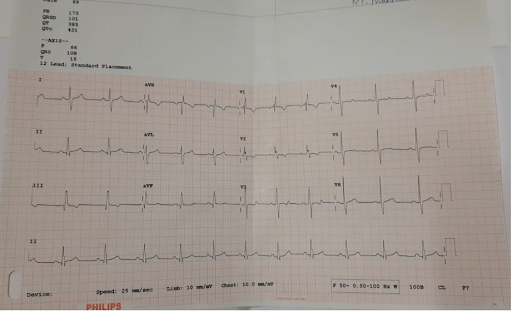
2. ECG: Incomplete Right Bundle Branch Block, consistent with ASD
3. Chest x-ray: Cardiomegaly

Lab investigation
- Hb – 11.3
- PCV – 39.7
- WBC – 7250
- Platelet – 282000
- PT – 16.8
- APT – 33.9
- Sodium – 138.0
- Potassium – 2.50
- Urea – 23.18
- Creatinine – 0.83
- Uric acid – 4.95
- Protein – 4.91
- SGPT – 20.90
- SGOT – 16.78
- Globulin – 1.31
- A/G Ratio – 2.75
- Triple H – Negative
Operational Notes
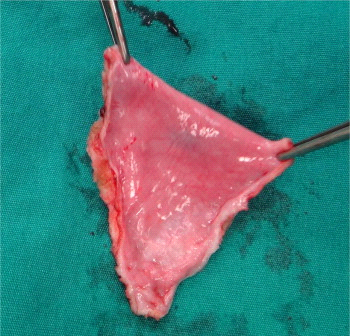
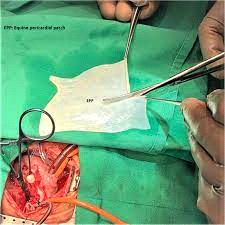
After a sternotomy the pericardium is dissected free of the fat and opened toward the left. Stay sutures are taken. After the standard protocol of cannulation and institution of cardiopulmonary bypass, the right atrium is opened and retracted to facilitate better exposure. A slit is made in the right flap of the pericardium, parallel to its free margin, at a distance equal to the width of the atrial septal defect. Using a 4-0 polypropylene double-arm done.
CT – ICU Care
- After surgery, patient was taken to the intensive care unit and monitored.
- Cardiac monitors – to monitor vital signs
- Patient with Mechanical ventilator support.
- Infusion pumps – e g. Inj. NTG, Inj. Doputamine, Inj. Nor adrenaline to regulate the Heart rate and BP.
- ICD tube connected with negative pressure suction.
- Pain medication given as appropriate.
- Inotropes slowly tapered and stopped.
- ICD Tube removed after 2 days.
- Patient hemodynamically stable and patient shifted to ward.
Treatment
- Inj. CETIL 750 mg BD
- Inj. Pan 40 MG od
- T. dytor 5 mg BD
- T. Conco 2.5 mg OD
- T. Dolo 650 mg TDS
- Neb Duolin TDS
- Neb Budecort TDS
Nursing Management
- Counselling given to the attenders related to post op care.
- Healthy dietary habit advised
- Wound kept clean and healthy
- Chest physio given
- Encouraged spirometry exercises
- I/O chart maintained.
- Early ambulation is done
- Educated the patient to avoid weight lifting.
Dietary advice
During the post-operative period clear liquid was given, followed by liquid diet is started. After that semi solid diet was given to patient, which was tolerated and after that advised to take normal diet as well as balance diet was provided.
Post OP ECHO: Optimum results
Outcome
On discharge, patient was hemodynamically stable.
Discharge Advice
- To monitor squeezing pressure, pain in the chest.
- To avoid lifting heavy objects, and rest when needed. Advised that it may take 6 to 8 weeks after surgery before one feels completely better.
- To ask family to help with daily activities.
- Carefully change bandages when they get wet.
- To take balanced diet.
- To do spirometer exercise and deep breathing exercise.
Reference
- Celermajer DS. Atrial septal defects: even simple congenital heart diseases can be complicated. Eur Heart J. 2018 Mar 21;39(12):999-1001.
- Aoki H, Horie M. Electrical disorders in atrial septal defect: genetics and heritability. J Thorac Dis. 2018 Sep;10(Suppl 24):S2848-S2853.
- van der Linde D, Konings EE, Slager MA, Witsenburg M, Helbing WA, Takkenberg JJ, Roos-Hesselink JW. Birth prevalence of congenital heart disease worldwide: a systematic review and meta-analysis. J Am Coll Cardiol. 2011 Nov 15;58(21):2241-7
- Behjati-Ardakani M, Golshan M, Akhavan-Karbasi S, Hosseini SM, Behjati-Ardakani MA, Sarebanhassanabadi M. The Clinical Course of Patients with Atrial Septal Defects. Iran J Pediatr. 2016 Aug;26(4):e4649.

Ms.Devi
Staff Nurse

Ms.Sheetal
Nursing Incharge
