Peri-operative care during Cytoreduction Surgery (CRS) with Hyperthermic Intraperitoneal Chemotherapy (HIPEC): Kauvery experience.
Valarmathi.M1, Sujitha2, Mahalakshmi3*
OT Incharge, Kauvery Hospital, Tennur
Scrub Nurse, Kauvery Hospital, Tennur
Nursing Superintendent, Kauvery Hospital, Tennur
Abstract
Cytoreduction surgery (CRS) with hyperthermic intraperitoneal chemotherapy (HIPEC the induced Hyperthermia which lasts for about 1-1.5 hr. Although the mortal) is considered as one of the most complex abdominal surgical procedure performed for diseases causing peritoneal carcinomatosis such as Pseudomyxoma peritonei, Ovarian cancers and colorectal cancers with peritoneal metastasis. The complexity and the high risk of post-operative mortality and morbidity is due to the prolonged procedure sometimes extending upto 12-16 hr, multi visceral resections and most importantly the homeostatic changes that happens during mortality and morbidity were high when these procedures when performed initially 2 decades back now it is performed safely with an accepted mortality of less than 4% and morbidity less than 20-30%. In this article we are sharing our experience from the nursing perspective how this procedure is performed and the standardized peri-operative care we provide for patients undergoing this procedure for a successful outcome.
Case Presentation
This is a 55 years old lady with no major comorbid evaluated for abdominal discomfort and suspected to have appendicular neoplasm hence referred to our center. After clinical assessment and imaging including CT scan abdomen and pelvis with tumor markers CA 19-9 and CA 125 (both were within limits) she was diagnosed with appendicular mucinous neoplasm with pseudomyxoma peritonei. She underwent Diagnostic laparoscopy for biopsy and peritoneal carcinomatous index (PCI) scoring. Diagnostic laparoscopy revealed gelatinous ascites in pelvis with peritoneal deposits in sub diaphragmatic peritoneum with PCI score of 20. Biopsy from the peritoneal disease confirmed to be positive for malignancy. She was planned for the definitive treatment Cytoreduction surgery (CRS) with HIPEC.
Pre-operative preparation
Patient and family members counselling and consent
Patient and the entire family members were described in detail the nature of the disease and the options of treatment including the complexity of the procedure, the risks involved and the expected outcome.
Patient and the family members were given enough time for them to make a decision understanding what they are going to undergo without any pressure but were reassured that all possible measures would be taken to perform the procedure safely and improve her health to be discharged home in good health.
Once the family members had agreed for the procedure a detailed video consent as well as a written consent of the same was recorded.
Rehabilitation
After getting appropriate cardiac and pulmonary fitness patient received pulmonary physiotherapy and rehabilitation exercise with Glutamine rich supplements which have all shown to improve post-operative recovery.
Bowel preparation and DVT prophylaxis
Bowel preparation done with Coloprep and DVT prophylaxis initiated the day before surgery.
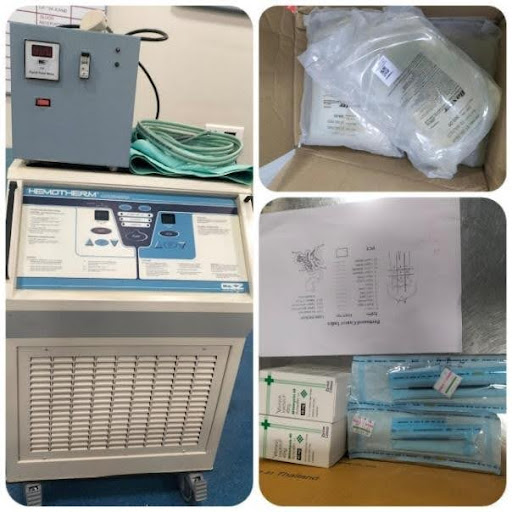
Arranging appropriate instruments and materials
Being a uncommon procedure some of the materials and instruments used during the procedure were not easily available hence we had made a check list for the materials and the instruments needed for the procedure and made sure all were arranged before the day of surgery. Some of the instruments that were used are
HIPEC machine: Used for infusing chemotherapy under hyperthermia.
Arranged from a third party vendor by rental agreement;
- Body warmer – A crucial gadget used to regulate the temperature of the patient during the period of hyperthermia in maintaining the core body temperature.
Arranged from our sister concern hospital;
- Mitomycin chemotherapy for infusion during hyperthermia.
- Peritoneal dialysis fluid – 1.5% Dextrose for Chemotherapy infusion.
- Book Walter retractors system.
- Staplers and suture materials.
- Ball tip diathermy pencil.
- Head light for better illumination.
- Smoke evacuators: To absorb the smoke during the use of diathermy and also the vaporized chemotherapy during the period of HIPEC.

Blood products
Adequate blood products including PRC, Platelets, FFP and most importantly Albumin infusions were arranged.
Surgical Procedure
- Induction and anesthesia – As with any other major surgical procedure patient had Central venous access, arterial lines and epidural catheter and was intubated after appropriate medications.
- Patient was positioned in Lithotomy using Stirrups and appropriate shoulder support with gel pads provided. WHO Safety check list is completed and along with it in view of the multiple steps involved in the procedure we had developed a check list made to avoid missing out any of the steps in the procedure which would be completed at the end of the procedure.
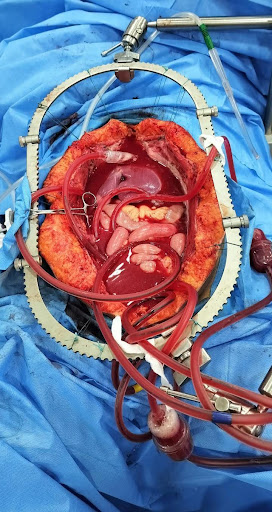
- Mid line laparotomy done and thorough examination of the entire viscera done to confirm the appendix tumor with peritoneal deposits and mucinous /gelatinous ascites. PCI scoring was around 20, hence decided to proceed with CRS with HIPEC as planned.
- Cytoreduction surgery (CRS) – Aim of cytoreduction is surgically remove all macroscopic disease and in this case the appendix with right colon and uterus with ovaries and the entire peritoneum.
Total Peritonectomy Completed in Five Parts
- Anterior parietal peritonectomy,
- Right subdiaphramatic peritonectomy,
- Left subdiaphramatic peritonectomy,
- Total omentectomy with omental bursectomy,
- Pelvic peritonectomy with bladder peritonectomy.
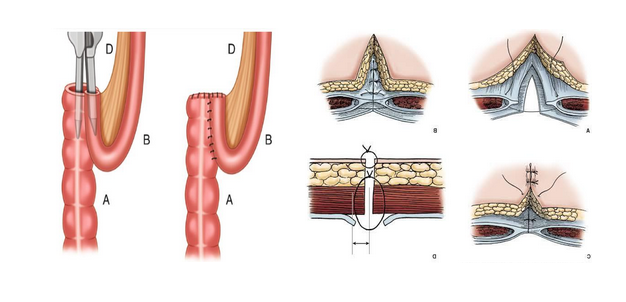
- Visceral resections included Right hemicolectomy,
- Hysterectomy with B/L Salphingo-oopherectomy and Cholecystectomy.
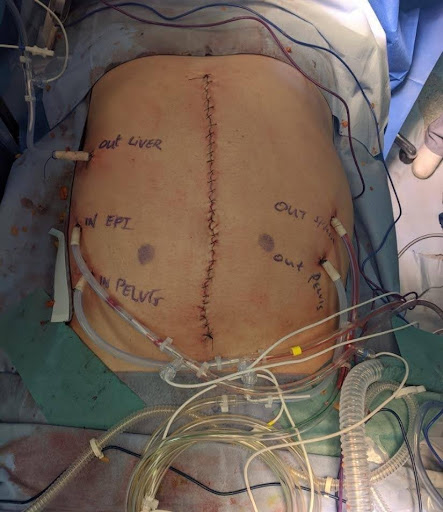
HIPEC

Aim of HIPEC to attack the microscopic disease with chemotherapy Mitomycin under hyperthermic condition for a period of 1 hour at 42°C. This period of induced hyperthermia is a challenge to the anaesthesia team in maintaining the homeostasis including the volume status of the patient which needs higher crystalloids infusion upto 3-7 ml/Kg body weight , multiple albumin infusions, Maintain adequate renal output , maintain appropriate core temperature in-spite of a higher intra- peritoneal temperature, electrolyte and blood sugar maintenance. ABG is performed every 15 min for maintaining Acid- base balance which in most cases have high lactate and acidosis.
Chemotherapy is circulated with the help of the HIPEC machine which maintains the set temperature of 42° with the use of drain tubes with built in thermostats. Appropriate measures taken to prevent contamination of the chemotherapy by spillage or by vapor including restriction of staff during HIPEC, appropriate protection gears and smoke evacuators to absorb the smoke.
After HIPEC a thorough saline wash is given followed by Ileo-colic anastamosis and abdominal wall closure after appropriate drains and Intercostal drains. Surgical step check list completed along with WHO safety check list and abdomen closed.
Total duration of the procedure was around 14 hours with a total blood loss of around 1500 ml which were replaced with.
Post-operative Care
Patients were electively ventilated overnight in ICU and extubated the next day after assessing the general condition and the ABG report.
Post-operative Day 1-2
Electively after extubation patients receive High flow nasal oxygen (HFNO) support for 48 hrs , Pain management through epidural catheters, high renal output of around 150 ml /hr is maintained to excrete the chemotherapeutic drugs, Total parental nutrition is started on day one along with antibiotic and proton pump inhibitors, anticoagulants are withheld as most patients will have a transient increase in coagulation profile with elevated transaminases which reduces by day 3. DVT stocking applied, Daily CBC, electrolytes, LFT, coagulation profile, albumin, X ray chest and ABG done till Day 3.Packed cell transfusions to maintain a hemoglobin level above 8 mg/dl and albumin infusion given to maintain a albumin level above 3 mg/dl.
Post-operative Day 3-5
Patient weaned from HFNO to room air, mobilised and shifted to post-operative care ward , Prophylactic anticoagulants started with pulmonary rehabilitation. Antibiotics stopped based on clinical condition and Serum procalcitonin levels which are performed on Post op day -3 and 5. Oral diet started gradually based on bowel movements and gradually increased over the Day 4-8 and TPN stopped.
Post-operative day 5-8
Patient shifted to ward and Drains , ICD tubes, Foleys, Epidural catheters , central lines removed , mobilized well , oral diet established and prepared for discharge.
Delayed immunosuppression due to chemotherapy is closely monitored by CBC and managed appropriately if present.
Conclusion
Although considered a complex procedure with challenges at various levels during the peri-operative period, CRS with HIPEC can be performed safely and a good outcome can be obtained consistently by good coordinated team work between the surgical team, anesthesia team, critical care team, surgical nursing staff and the post-operative nursing staff. Standardisation of the entire process from pre-operative preparation to intra operative surgical steps and post-operative care by breaking it into smaller steps with standard operating procedure for each step along with checklists and pathways makes this prolonged and complex procedure to be performed safely with very low mortality and morbidity to obtain a good outcome.

Team members
Surgeons and Anaesthetists
- Dr. Anis. B, MBBS, MS, MRCS, MCh
- Dr. Surendrakumar. G, MS, MCh (Surgical oncologist)
- Dr. Senthilkumar. K, MD (Anes),FIPM,PGOMILE (Anaesthesiology)
- Dr. Nirmalkumar. S, MBBS,DA,DNB (Anaesthesiology)
- Dr. Mohammed Iliyas. N, MD, DA, DNB (Anaesthesiology)
- Sr. Valarmathi. M (Nursing Incharge)
- Sr. Gayathri (Scrub nurse)
- Sr. Sujitha (Scrub nurse)
- Sr. Abinaya (Circulatory nurse)
- Sr. Lalitha (Anes.Technician)
- Mr. Dhanasekar (Anes.Technician)
Acknowledgement
- Dr. Senthilkumar.G
- Dr. Ramamoorthy for mentoring the procedure
