
A 69-year-old male patient who is a known diabetic for past 25 years and hypertensive for past 8 years, had h/o upper respiratory tract infection following which he developed decreased urine output for 5 days, pedal oedema and facial puffiness for 3 days and sudden onset breathlessness for which he got admitted in nearby hospital and treated as acute pulmonary oedema. 2D Echo showed normal LV function with EF-65%.CT abdomen showed normal size kidneys, bilateral perinephric fat stranding with no hydroureteronephrosis and mild prostatomegaly. Renal function worsened from creatinine of 1.9 to 4.4 in 2 days and patient became oliguric. Hence patient was referred to nephrologist. He was admitted in ICU, with Hb-8.8gm, urea-79mg, creatinine-4.6gm, Urine spot PCR-1.39. Serology was negative. CPK, CPK-MB were not high. In view of rapidly progressive renal failure and oliguria, he was initiated on Haemodialysis. Totally 4 sessions of dialysis were done on alternate days. ANA, c-ANCA, p-ANCA, Anti-GBM Ab were negative.
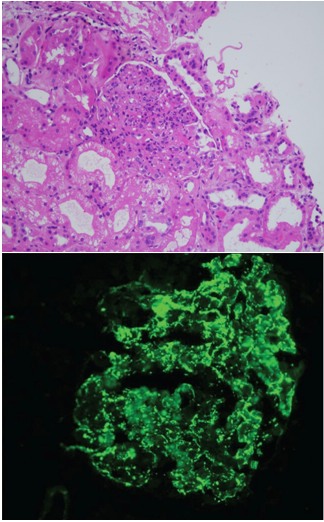
Renal biopsy was done. It showed under light microscopy five glomeruli which were identified. The viable glomeruli are hypercellular with endocapillary proliferation and neutrophilic infiltration. There was diffuse increase in mesangial matrix. No spike or crescent formation. Under Immunofluorescence C3(+3) and IgA (+2) shows granular positivity on the glomerular capillary loops. IgG (+1) shows linear positivity on the glomerular capillary loops. Renal biopsy report was suggestive post infectious glomerulonephritis with IgA dominance and diabetic nephropathy. Patient was pulsed with Inj. Methyl prednisolone 500mg IV OD for 3 days. Patient became symptomatically better with resolution of edema and there was adequate urine output. He was discharged with oral steroids (Prednisolone 1mg/kg) and on subsequent op follow up, serum creatinine was on the decreasing trend. Patient didn’t require further dialysis, hence dialysis catheter was removed.
Review of literature:
 IgA dominant acute post infectious glomerulonephritis (APIGN) is an morphologic variant of APIGN, particularly in the elderly1. In contrast to classic APIGN, in which there is typically glomerular deposition of IgG and C3 or C3 only, IgA is the sole or dominant immunoglobulin in IgA-dominant APIGN. Majority of the reported cases occur in association with staphylococcal infections, so alternatively designated as “IgA-dominant acute post staphylococcal glomerulonephritis” .Diabetes is a major risk factor, likely reflecting the high prevalence of staphylococcal infection in diabetics. Patient typically presents with severe renal failure, proteinuria and hematuria2. Prognosis is guarded with less than a fifth of patients recovering renal function. Nasr et al., in his review noted that only 16% of IgA APIGN had full recovery of renal function (≤1.2 mg/dl) whereas 43% had persistent renal dysfunction and 41% progressed to end-stage renal disease (ESRD)3. The prognosis of IgA PIGN is less favourable than that of typical APIGN. In our patient, there is partial recovery of renal function with creatinine pf 1.6 mg/dl and now on tapering dose of steroids. He is off hemodialysis currently.
IgA dominant acute post infectious glomerulonephritis (APIGN) is an morphologic variant of APIGN, particularly in the elderly1. In contrast to classic APIGN, in which there is typically glomerular deposition of IgG and C3 or C3 only, IgA is the sole or dominant immunoglobulin in IgA-dominant APIGN. Majority of the reported cases occur in association with staphylococcal infections, so alternatively designated as “IgA-dominant acute post staphylococcal glomerulonephritis” .Diabetes is a major risk factor, likely reflecting the high prevalence of staphylococcal infection in diabetics. Patient typically presents with severe renal failure, proteinuria and hematuria2. Prognosis is guarded with less than a fifth of patients recovering renal function. Nasr et al., in his review noted that only 16% of IgA APIGN had full recovery of renal function (≤1.2 mg/dl) whereas 43% had persistent renal dysfunction and 41% progressed to end-stage renal disease (ESRD)3. The prognosis of IgA PIGN is less favourable than that of typical APIGN. In our patient, there is partial recovery of renal function with creatinine pf 1.6 mg/dl and now on tapering dose of steroids. He is off hemodialysis currently.
The diagnostic features include initial presentation in older age, diabetic patient, acute renal failure, intercurrent culture-documented staphylococcal infection, hypocomplementemia, diffuse glomerular endocapillary hypercellularity with prominent neutrophil infiltration on LM, stronger IF staining for C3 than IgA and subepithelial humps on EM4,5. Hence greater awareness of this entity among renal pathologists and nephrologists is needed to distinguish this condition from the more common entity of IgA nephropathy.
REFERENCES:
1. Brenner and Rector’s The Kidney – Eleventh Edition
2. Nasr SH, Fidler ME, Valeri AM, Cornell LD, Sethi S, Zoller A, et al. Postinfectious glomerulonephritis in the elderly. J Am Soc Nephrol. 2011;22:187–95.
3. Nasr SH, D’Agati VD. IgA-dominant postinfectious glomerulonephritis: A new twist on an old disease. Nephron Clin Pract. 2011;119:c18–25.
4. Montseny JJ, Meyrier A, Kleinknecht D, Callard P. The current spectrum of infectious glomerulonephritis: Experience with 76 patients and review of the literature. Medicine. 1995;74:63–73.
5. Nasr SH, Markowitz GS, Whelan JD, Albanese JJ, Rosen RM, Fein DA, et al. IgA-dominant acute post staphylococcal glomerulonephritis complicating diabetic nephropathy. Hum Pathol. 2003;34:1235–41
 Dr. Balaji Kirushnan
Dr. Balaji Kirushnan Dr Vishnu
Dr Vishnu
{kind=link}