
Abstract
Spleen injuries are among the most frequent trauma-related injuries. At present, they are classified according to the anatomy of the injury. The management of splenic trauma patients aims to restore the homeostasis and the normal pathophysiology especially considering the modern tools available for bleeding management. Thus, the management of splenic trauma should be based on the physiology of the patient, the anatomy of the injury, and the associated lesions.
Keywords
Splenic injury, non-traumatic, CT Abdomen, left shoulder pain, pain abdomen, splenic rupture
Case Presentation
A 75 years Lady Known case of hypertension, Type 2 diabetes mellitus, left pyelonephritis with HUN -S/P Cystoscopy and DJ stenting was done two weeks back. Now came to our emergency department with complaints of abdominal pain, diffuse, left side, Iliac region, non-radiating since that day afternoon. She also had pain in Left arm, pricking type, non-radiating. She had no history of trauma, chest pain, palpitations, breathing difficulty, giddiness, loss of consciousness, excessive sweating, seizure, ENT bleeding, fever, cough, cold, nausea, vomiting, loose stools, decreased urine output or hematuria.
No history of any trauma in the past.
On receiving her in Emergency department she was conscious, oriented, afebrile, hydration was fair with blood pressure of 190/80mmhg, pulse 84/min, respiration22/min, capillary blood glucose was high and temperature of 96°F. She had no pallor, icterus, cyanosis, clubbing, lymphadenopathy or pedal edema.
On Systemic Examination
Respiratory system: bilateral air entry with fine basal crepitations.
Cardiovascular system: S1S2 heard, no murmur.
Per abdomen: revealed tenderness predominant in epigastric region and left Iliac region. Umbilical hernia present. Bowel sounds heard.
Per rectum examination: soft stools, no blood stains, fissure.
Routine investigation were done.
Investigation and management:
VBG:
pH:7.41
Pco2:31.1
Po2:49
HCO3:20.1
Lac:0.93
Electrolytes:
Sodium:116
Potassium:5.7
Chloride:87
iCa:20
Glucose: >700
BUN:28
Cr:1.2
Hb: 11.2
White Blood Cells: 8800
N:81.4
L:7.8
M:9.8
Platelet:407000
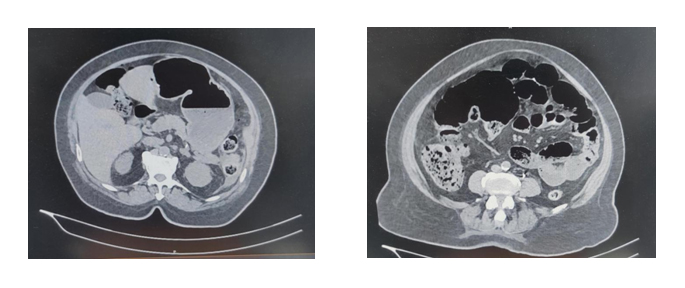
CT Abdomen: Interval appearance of multiple hypoechoic areas with air pockets within the spleen with surrounding fluid. Interval resolution of air pockets within the left pelvicalyceal system and fecal loaded large bowel.
ECHO: No RWMA
Normal LV Systolic Dysfunction (LVEF=60%)
Trivial AR/MR
Normal RV Size and function
Tachycardia noted during study(HR:103)
Normal size IVC
ECG: Heart rate:80/min, normal sinus rhythm, normal axis, normal interval
No significant ST /T changes.
In view of persisting pain, he was administered with analgesics and proton pump inhibitor.
In view of glucose >700, but patient’s blood gas didn’t show evidence of acidosis, hence she was started on insulin infusion at 6ml/hr after obtaining diabetologist’s opinion for glycemic control.
Expert gastroenterologist opinion obtained and patient was planned for laparotomy and proceed. During the procedure, she was found to have splenic rupture and immediate splenectomy was done along with ventral hernia repair. Post-operative period was uneventful.
She improved and was symptomatically better hence discharged with oral medication and when she was reviewed after one month, she was asymptomatic and hemodynamically stable.
Discussion
Splenic rupture can be divided into two major categories: traumatic and non-traumatic rupture. The most prevalent major mechanism in traumatic injury (50% to 75%) is the result of motor vehicle injury. Direct abdominal blows and falls are the remaining major causes of traumatic rupture. Additionally, traumatic rupture can present immediately after an injury or may present in a delayed fashion.
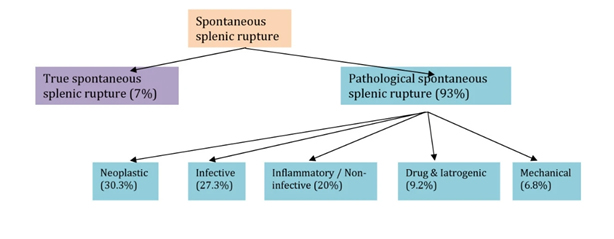
Non-traumatic splenic rupture is very uncommon, though can be related to underlying pathologic conditions or may be idiopathic.
A splenic injury may not always be clinically apparent, even in the background of insignificant or negligible trauma there could be splenic injury & rupture. A high index of suspicion is always warranted.
Ultrasound can be very helpful and highly accurate in the diagnosis of significant splenic injury and it can be used in the ED to detect even minimal amounts of fluid in the abdomen via an EFAST scan, even up to 100 ml in abdomen can be detected.
CT Scan has become the mainstay of stable patient evaluation since it can provide splenic injury severity and assessment of other abdominal organs.
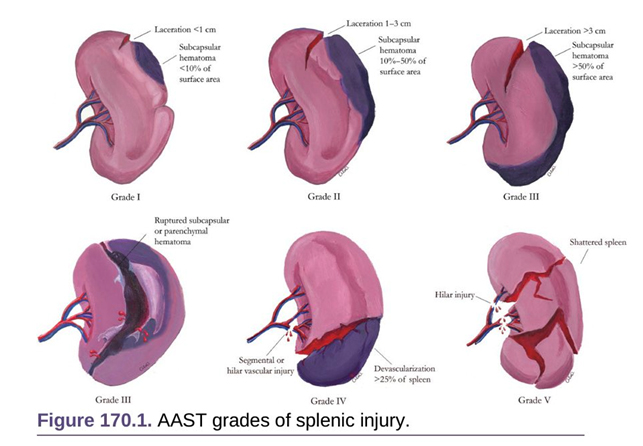
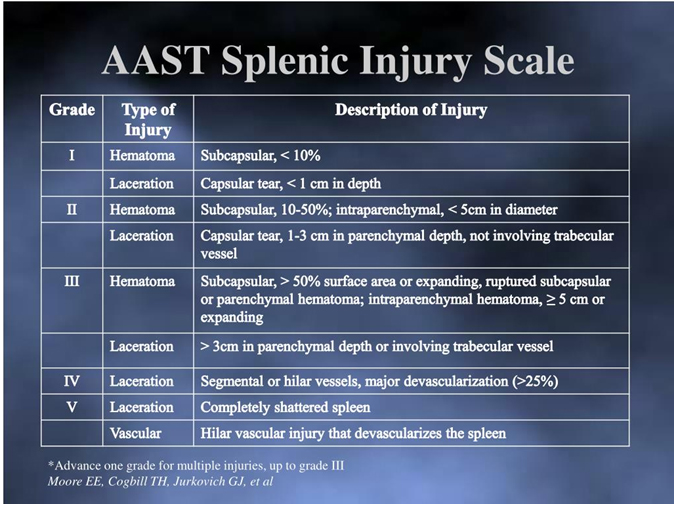
Splenic injury is classified based on CT findings according to the American Association for the Surgery of Trauma (AAST) Organ Injury Scale. It helps categorizes splenic injuries but does not predict the need for surgical intervention.
CONCLUSION
Unexplained left arm pain associated with left sided abdominal pain must raise a suspicion of possible splenic injury.
Multiple air pockets around the spleen on imaging should raise suspicion of a spontaneous splenic rupture in the absence of trauma.
Grading of splenic injury and an aggressive management is required to reduce the overall mortality and morbidity of the patient.
Acknowledgments:
I would like to thank, Dr.Aslesha (Consultant and Clinical Lead Emergency Department)
For guiding me with the article.
“The authors declare no conflict of interest.”
References
- Kyriacou, A., Arulraj, N. & Varia, H. Acute abdomen due to spontaneous splenic rupture as the first presentation of lung malignancy: a case report. J Med Case Reports5, 444 (2011). https://doi.org/10.1186/1752-1947-5-444
- Gaillard, F., Jones, J. AAST spleen injury scale. Reference article, Radiopaedia.org. (accessed on 12 Jul 2022) https://doi.org/10.53347/rID-2074
 Dr.Mohammed Rashid Abdul Khader
Dr.Mohammed Rashid Abdul Khader
2nd year MRCEM Resident
Department of Emergency Medicine
Kauvery Hospital Chennai
