
A 77 year-old male came with complaints of fever with chills and rigor, seizure and generalized fatigue.
Patient underwent MRI. MRI image shows T2/FLAIR hyperintensities with diffusion restriction and low ADC values seen in ventral pons extending to both middle cerebellar peduncles, sulcal space of bilateral medial frontal lobes in the pericallosal gyrus .Post contrast images showed small conglomerate ring-enhancing lesions largest measuring 5.6 x 5.5 mm in both medial frontal lobes with meningeal enhancement. Meningeal enhancement was also noted along the ventral pons and middle cerebellar peduncles. Diffusion restriction with T2/FLAIR hyperintensity seen in right medial thalamus. In post contrast FLAIR images, it showed subtle meningeal enhancement. These features suggest infective etiology, more towards tuberculous etiology.
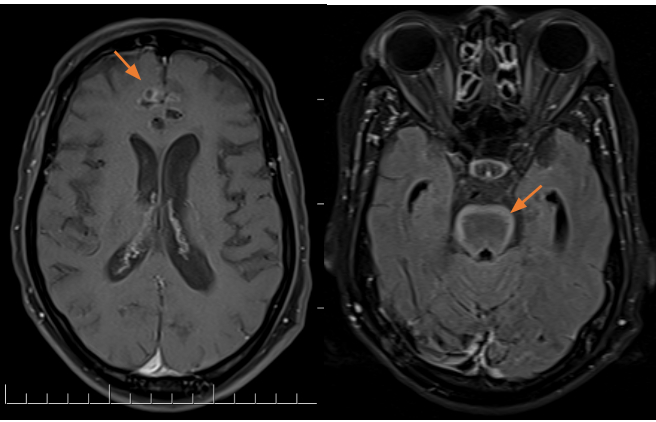
1. Axial section of CE-MRI A) T1 w image shows ring enhancing lesion in right medial frontal lobe (red arrow) B)Post contrast FLAIR shows meningeal enhancement along the ventral pons (red arrow).
CSF analysis include Adenosine Deaminase , Gene Xpert was negative.
Patient underwent CT for some other reasons. Incidentally noted, a well-defined soft tissue dense mass lesion in posterior segment of left lower lobe of size 3.4 x 2.8 x 3.6 cm with broad base towards pleura and abrupt cut off of posterior segmental bronchi.
Another similar soft tissue dense nodule in superior segment of left lower lobe size 1.4 x 1 x 2.3 cm. The possibilities include primary lung malignancy, metastasis.
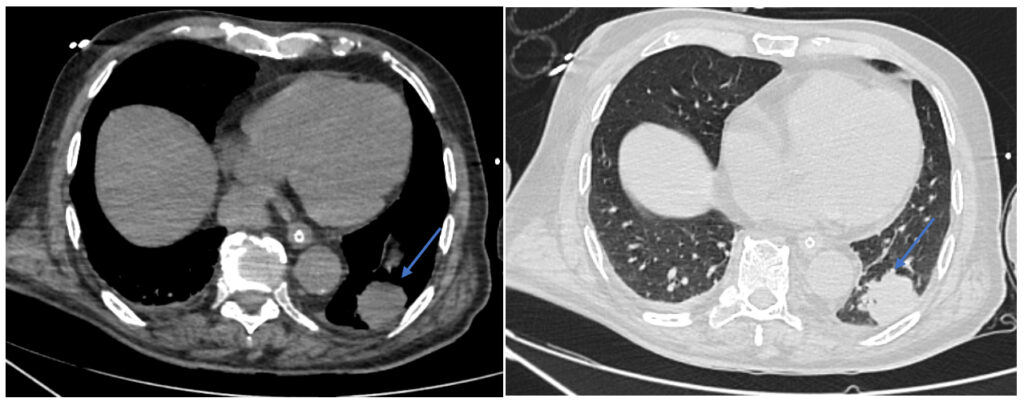
2. Axial sections of CT-chest mediastinal and lung window soft tissue density mass lesion in posterior segment of left lower lobe (blue arrow)
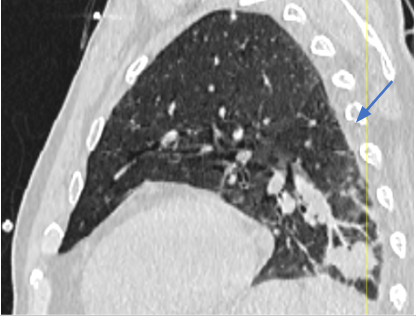 3. Sagittal section of CT chest shows lesion with abrupt cut off with posterior segmental bronchus (blue arrow).
3. Sagittal section of CT chest shows lesion with abrupt cut off with posterior segmental bronchus (blue arrow).
Initially, we thought the patient had infectious etiology, possibly tuberculosis. After the negative result of Gene Xpert and the CT-CHEST, which shows a mass in the posterior segment, the diagnosis changed. The lesions in brain and meningeal enhancement in the background of chest mass, suggest a different diagnosis. The diagnosis is now more likely to be metastasis, specifically leptomeningeal carcinomatosis. This is due to the presence of chest mass and meningeal enhancement, which are not typical of tuberculosis.
The diagnosis is now more consistent with leptomeningeal carcinomatosis, a common complication of metastatic cancer.
 Dr. Firdhous
Dr. Firdhous Dr. Roopini
Dr. Roopini Dr. Kanagasabai K
Dr. Kanagasabai K Dr. Sivarajan Thandeeswaran
Dr. Sivarajan Thandeeswaran
{kind=link}