INTRODUCTION
Infection related glomerulonephritis (IRGN) is an immune mediated glomerulonephritis mediated by alternate complement pathway activation by bacterial,viral or parasitic infections.
AIM
To determine the clinical spectrum,nature of infection,renal histology, use of immunosuppressants and outcome of patients with biopsy proven IRGN.
MATERIALS AND METHODS
This is a retrospective observational study. The data of a total of 17 native kidney biopsies of patients with IRGN were studied for their clinical characteristics, renal histology, treatment and outcomes.
RESULTS
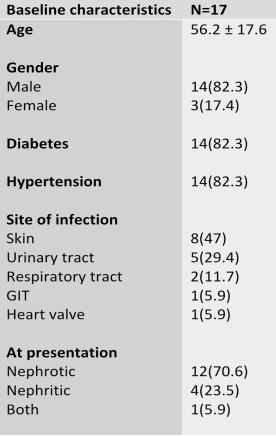
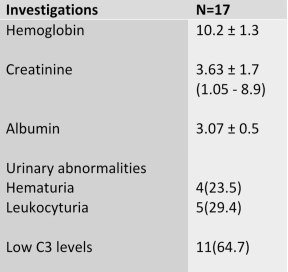
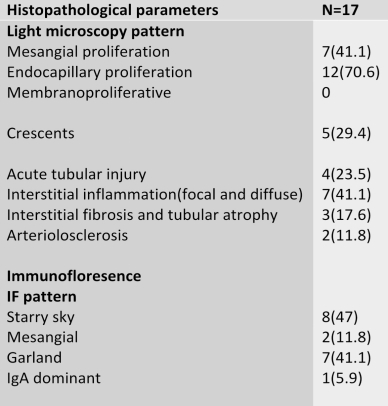
The mean age of presentation was 56.2 ± 17.6 years with a male preponderance. The serum creatinine level at presentation ranged from 1.05- 8.9mg/dl. A nephrotic range of proteinuria was seen in 70.6% of cases. The most common histological presentation included Mesangial (41.1%) and endocapillary (70.6%) proliferation. One out of 17 cases was proven to be IgA dominant IRGN. The site of infection was predominantly skin (47%), 29.4% from urinary tract. 76.4% of patients were treated with steroid alone and 23.5% with steroid and other immunosuppressants. 70.6% of patients had remission and 23.5% required hemodialysis.

DISCUSSION
Infection-related glomerulonephritis encompasses the entities of postinfectious (poststreptococcal) GN, immunoglobulin IgA dominant, (Staphylococcus-associated) endocarditis associated IRGN and shunt nephritis. [1] The pathophysiology of IRGN includes the deposition complement associated with or without immunoglobulin deposition by various mechanisms like entrapment of circulating immune complex, immune complex formation in situ or independent complement activation by bacteria.
The sites of adult infection are more heterogeneous including skin, upper respiratory tract, urinary tract, lung,heart, oral mucosa/teeth with few harbouring infection at more than one site. The clinical spectrum of IRGN may vary from asymptomatic microscopic hematuria incidentally detected on urine analysis to rapidly progressive glomerulonephritis requiring emergency hemodialysis. [2]Serum creatinine is elevated in most of the patients at presentation. A low C3 level is seen in majority of patients. Severe renal failure requiring dialysis is seen in elderly patients. Endocapillary glomerular hypercellularity with neutrophils may give the first clue for diagnosis of IRGN. Immunofluorescence would show C3 deposition with or without immunoglobulins.[3]Patterns of staining in the setting of IRGN include the “garland,” “starry-sky,” and “mesangial” patterns. The management of IRGN must include antibiotics to eradicate infection, diabetic and hypertension control, diet salt restriction, diuretics if required. Immunosuppressants such as steroid, mycofenolate have been shown to induce remission in these patients. Renal replacement therapy for rapidly progressive renal failure to manage complications like pulmonary oedema, hyperkalaemia and uraemia symptoms.
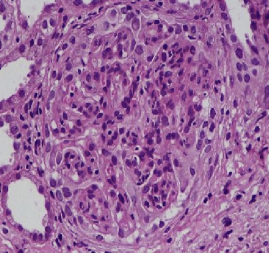
Endocapillary hypercellularity in light microscopy
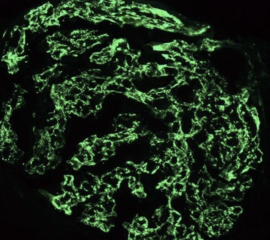
Starry sky appearance on immunoflurescence

Garland pattern on immunoflurescence
REFERENCES
- Nasr SH, Markowitz GS, Stokes MB, Said SM, Valeri AM, D’Agati VD. Acute postinfectious glomerulonephritis in the modern era: experience with 86 adults and review
- Kambham N. Postinfectious glomerulonephritis. Adv Anat Pathol. 2012; 19(5): 338–47.
- Hunt EAK, Somers MJG. Infection-related glomerulonephritis. Pediatr Clin North Am. 2019; 66(1): 59–72.
 Dr Yashilha D
Dr Yashilha D Dr R Balasubramaniyam
Dr R Balasubramaniyam Dr B Balaji Kirushnan
Dr B Balaji Kirushnan
{kind=link}