
Case Report
Mr. X, a 47-year-old male, presented to the neurology outpatient department with a two-month history of left-sided chest pain radiating to the back. The pain was insidious in onset, intermittent, pricking in nature, and aggravated by movement or lying on the left side. Relief was noted with massage or adopting a flexed posture. The pain was associated with occasional dyspnea and a catching sensation during breathing. The pain did not respond to standard analgesics. He also had similar complaints 2 years ago, later resolved spontaneously.
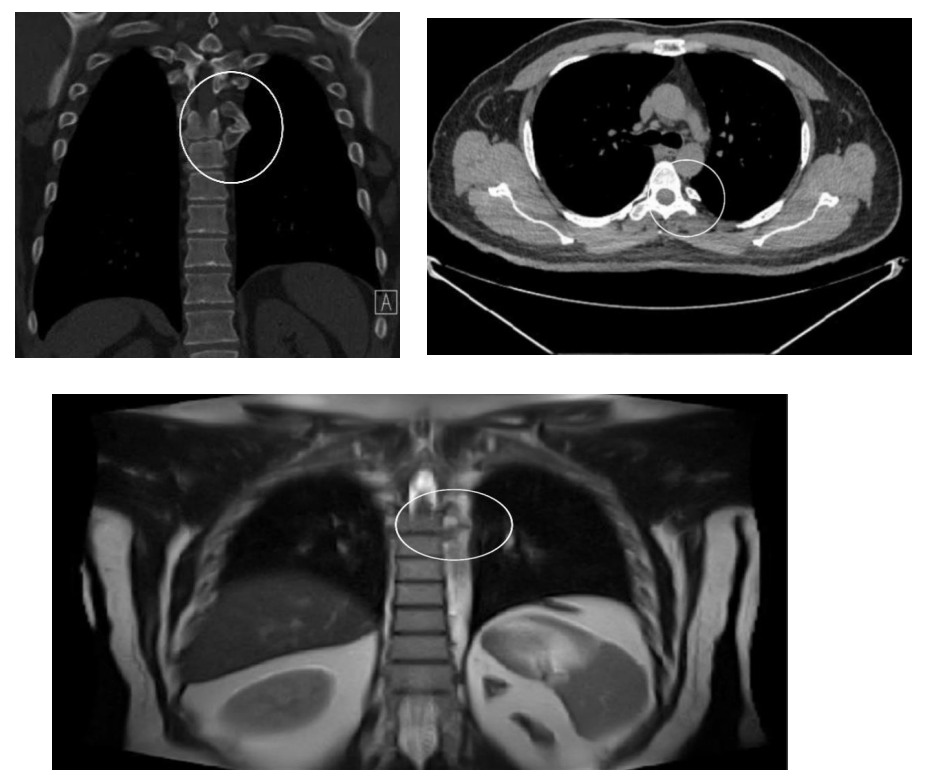
Initial consultations included an orthopedic evaluation where an MRI of the chest and spine was performed. The results were unremarkable, and analgesics were prescribed, which did not give relief to the patient. Further evaluations with a Cardiologist and Gastroenterologist ruled out Cardiac and Gastric causes of pain, including a CT scan of the chest and abdomen, which were normal.
Upon detailed neurological examination, no abnormalities were observed in the overlying skin. There was no warmth or tenderness, but the pain demonstrated a characteristic distribution along the D5 dermatome. This dermatomal pattern raised suspicion of a structural anomaly, prompting a reevaluation of the CT chest images in collaboration with a radiologist. A pseudoarticulation between the fifth and sixth ribs was identified, likely accounting for the patient’s symptoms.
Management
In this case, the dermatomal distribution of pain served as a crucial clinical clue. The patient was prescribed Tab. Pregabalin to manage neuropathic pain and advised to review his symptoms after a few days. If the symptoms not resolving then a Nerve block is to be planned.
Discussion – Pseudoarticulation of Ribs- Leading to Intercostal Neuralgia
Pseudoarticulation of a rib refers to an uncommon anatomical variation in which an abnormal joint-like structure forms between a rib and an adjacent bone or another rib. This condition can arise from congenital anomalies, developmental disturbances, or acquired factors such as trauma. It is most commonly observed in the first rib, but other ribs may also be involved. Pseudoarticulation is typically identified incidentally on imaging studies, as it is often asymptomatic.
Pathophysiology
Pseudoarticulation develops due to incomplete ossification or fusion of a rib during embryogenesis, leading to a fibrous or cartilaginous connection. Alternatively, it can result from repetitive stress or mechanical forces causing the development of an atypical articulation over time. The intercostal nerves, which run along the inferior border of each rib within the costal groove, are vulnerable to compression or irritation from structural abnormalities like bone deformities, pseudoarticulations, fractures, or tumor growth. Abnormalities such as rib pseudoarticulations or fractures can exert direct pressure on the intercostal nerves.
Clinical Presentation
While most cases are asymptomatic, pseudoarticulation may present with:
- Localizedpain due to mechanical
- Neurological symptoms from compression of adjacent nerves, particularly in cases involving the thoracic outlet.
- Restricted range of motion or deformities in severe cases.
Diagnosis
Imaging modalities play a key role in diagnosing pseudoarticulation:
- X-ray: Often the first-line investigation, revealing an abnormal articulation orbony prominence.
- CT Scan: Provides detailed visualization of the bony anatomy and joint formation.
- MRI: Useful for evaluating soft tissue involvement and potential nerve
 Management
Management
Treatment is typically conservative unless symptomatic:
- Observation: Asymptomatic cases require no
- Pain Management: NSAIDs and physiotherapy, Nerve block may alleviate
- Surgical Intervention: Reserved for cases with significant pain, neurological
compromise, or cosmetic concerns. Resection of the pseudoarticulation may be considered. Radio-frequency ablation or dorsal root ganglion treatments in refractory cases.
Conclusion
Intercostal Neuralgia and Pseudoarticulation of ribs should be considered in the differential diagnosis of chronic, radiating chest pain unresponsive to conventional treatment.
References
- Brazis, P.W., et al. (2021). Localization in Clinical Neurology – Discusses mechanisms of nerve compression and neuropathic pain.
- Online Medical References:
- UpToDate articles on “Intercostal Neuralgia” or “Chest Wall Pain Syndromes.” https://www.uptodate.com/contents/ management-of- isolated-musculoskeletal-chest-pain
- Intercostal Neuralgia – Dalton Fazekas; Maksym Doroshenko; Danielle B. Horn https://www.ncbi.nlm.nih.gov/books/ NBK560865/
 Dr Vignesh A S, MBBS,
Dr Vignesh A S, MBBS,
DNB General Medicine Resident,
Kauvery Hospital Chennai
 Dr. Bhuvaneshwari Rajendran
Dr. Bhuvaneshwari Rajendran
M.B.B.S., M.R.C.P.(UK), C.C.T.(UK), DIP UCL-UK-Neurology
Senior Consultant Neurologist,
Kauvery Hospital Chennai

{kind=link}