Authors:- Dr N Sekar, Dr Jithin Jagan S, Dr Rahul R Sima, Dr Archana G
Department of Vascular and Endovascular Surgery, Kauvery Hospital, Chennai
Abstract
The chronic mesenteric ischaemic disease is becoming commonplace in the Indian scenario along with coronary arterial disease, peripheral vascular disease, and carotid arterial stenotic disease. Here we present a case of a 68-year-old lady who presented with abdominal pain and “food fear”. She had a loss of appetite and weight over a period of nine months. Ct angiogram carried out revealed a “shaggy” atherosclerotic aorta with bilateral renal artery stenosis and stenosis/occlusion of all three mesenteric vessels. She was diagnosed to have chronic mesenteric ischaemia and underwent an open retrograde ileo-mesenteric bypass. Post-operative period was complicated by paralytic ileus, and she developed unstable angina which was managed medically. She recovered well and was later discharged on the 9th post -operative day. She is doing well six months post-surgery.
Introduction
Chronic mesenteric ischaemia is a burgeoning problem in India. There is an increasing incidence of mesenteric ischaemia in patients with cardiac, peripheral vascular, carotid, and renal arterial disease. Timely treatment of these patients prevents progression to acute on chronic ischaemia and a mortality of 40%1. Patient selection and pre-, intra-, and post-operative decision-making play an important role in managing these patients successfully. Most of these patients have impairments in two or more vascular beds, making treatment of these patients challenging. We present here a case of chronic mesenteric ischaemia with concomitant coronary artery disease and peripheral vascular disease managed surgically with help from our anaesthesia, cardiology, and intensive care teams.
Case Report
History and Physical Examination
A 68-year-old female presented to the vascular surgery department with diffuse, intermittent upper abdominal pain complaints. There was pain when taking food and relieved after some time. The pain was dull-aching and not relieved by analgesics or acid suppressants. The pain persisted over a period of nine months and was unrelenting. She had visited several hospitals for the same. She also had claudication of her left lower limb, which started before to these complaints. She developed a “fear of food” resulting in a loss of appetite and weight. She had lost 15 kilograms in 6 months from symptom onset. She had one episode of melena eight months ago with persistent decreased bowel habits, which she attributed to decreased intake. She was a hypertensive person controlled on medication. She also gave a history of coronary artery disease.
On examination, she was poorly built and nourished. Her vitals were stable with a blood pressure of 150/80mm Hg. Her abdomen was scaphoid, diffusely tender with a bruit audible in the epigastric region. She also had a left renal angle bruit. Her femoral pulses were present, but the rest of her lower limb pulses were absent with monophasic flow in both her posterior tibial arteries.
Investigation
As her renal parameters were within normal limits, a CT aortogram was done. The aortogram showed an irregular, atheromatous abdominal aortic wall with moderate to severe stenosis of the left renal artery (Fig 1). The right kidney was non-opacified. There was a short segment occlusion for a length of 2.5cms in the superior mesenteric artery (SMA) from the ostium(Fig: 2). The coeliac artery had anostial stenosis with post-stenotic dilatation. A well- collateralised gastro-duodenal arcade (Arc of Buhler) was visualised. The inferior mesenteric artery(IMA) was also stenosed with well-developed meandering mesenteric artery(Arc of Riolan). The mesenteric circulation was well collateralised on CT between the coeliac, SMA and IMA (Fig: 1,2).
Diagnosis and Treatment
The patient was diagnosed to have chronic mesenteric ischaemia secondary to atherosclerotic disease with well-developed intrabdominal collaterals. As the patient did not improve with medical management, it was decided to intervene. Taking into account the “shaggy” nature of the aorta (Fig: 1) and distal peripheral vascular disease, it was decided to proceed with open mesenteric revascularisation instead of an endovascular approach. On evaluating her cardiac status, she was found to have moderate left ventricular dysfunction with an ejection fraction of 40%. A cardiology opinion was sought, and she was adequately optimized prior to surgery.
Procedure
Under general anaesthesia supplemented with an epidural, she underwent open mesenteric bypass procedure. The infra-renal aorta and left common iliac artery were heavily calcified, and the bowels were pale with a feeble pulse in the mesenteric and hepatic arteries (Fig 3). The right common iliac artery which was soft and compressible (disease-free) was planned as the inflow for the procedure. On dissecting the SMA, it was small in calibre with a heavily calcified occlusion in the proximal part. It had reformed from the middle colic branch and was patent distally. A right ileo-mesenteric bypass was carried out with 6×20 Goretex (PTFE vascular graft – Gore medical) graft(Fig 3). Post anastomosis, good pulsatile flow was seen in the hepatic artery, and hence a coeliac bypass was abandoned.
Post Procedure and Follow-up
The patient had postoperative ileus for 4 days which settled with adequate fluid management. The patient developed unstable angina on the 6th post-operative day, which was treated by nitrate infusion, and she improved. She was discharged on the 9th post-operative day on single antiplatelet and low-dose anticoagulant. She was maintained on oral nitrates for her unstable angina. On subsequent follow-up, her appetite improved with regular bowel habits. She is symptom-free for six months after the surgery and is on regular follow-up.
Discussion
Mesenteric vascular disease is a rare occlusive vascular disease with an incidence of 6 per lakh population 1. The exact incidence of CMI is not known, and neither is its prevalence in India. CMI has a very insidious course as seen in our patient2. These patients have very vague symptoms, and diagnosis is usually difficult clinically as they mimic several other intra-abdominal pathologies. A high index of suspicion is needed to diagnose the disease. There is a high prevalence of CMI in patients with coronary artery disease3. Diabetes, mesenteric angina and peripheral vascular disease were found to be independent predictors of CMI. Our patients had both CAD and PVD putting her at high risk of mesenteric vascular disease. In patients with CAD, PVD, or significant renal artery stenosis (>75%)4, a history of abdominal pain should be investigated further. The most common cause is atherosclerosis resulting in ostial narrowing of the mesenteric vasculature.
Most of these patients with CMI have a very stable disease3. Patients who have stable asymptomatic mesenteric disease have incredibly low incidence of adverse cardiovascular outcomes or mortality5. Hence radiologically positive but clinically negative patients need no further intervention5. Despite this, a subset of patients with asymptomatic disease develop acute mesenteric ischaemia as pointed out by Thomas JH et al6. Symptomatic patients with no respite from medical therapy need to undergo some form of revascularisation 3,7,8. There are multiple methods of revascularisation9 as listed below-
Open Approach
- Antegrade aorto-mesenteric bypass
- Retrograde aorto-mesenteric bypass
- Retrograde ileo-mesenteric bypass
- Re-implantation of mesenteric vessels
Endovascular Approach
- Coeliac angioplasty + stenting
- SMA angioplasty + stenting
Hybrid Approach
- Retrograde open mesenteric stenting
As the right common iliac artery was disease free in our patient, it was decided to carry out an ilio-mesenteric bypass. Endovascular and hybrid approach can be carried out for short segment ostial lesions with a disease-free aorta. Complications in the post-operative period are common and as high as 40% 10. Prolonged ileus secondary to reperfusion, as in our patients, is common with an incidence of 6%10. Cardiac complications are seen in 10% of the patients10. Open revascularisation has similar mortality rates to endovascular albeit with slightly higher morbidity. There is a higher rate of reintervention and restenosis with endovascular repair 10.
Conclusion
CMI should be diagnosed early and mesenteric revascularisation carried out in a select group of symptomatic patients not responding to medical therapy. The method of revascularisation should be individualised based on the extent and nature of the disease. Post-operative complications are common and have to be addressed promptly in this patient cohort.
References
- Zettervall SL, Lo RC, Soden PA, Deery SE, Ultee KH, Pinto DS, Wyers MC, Schermerhorn ML. Trends in treatment and mortality for mesenteric ischemia in the United States from 2000 to 2012. Annals of vascular surgery. 2017 Jul 1;42:111-9.
- Herbert GS, Steele SR. Acute and chronic mesenteric ischemia. Surgical Clinics of North America. 2007 Oct 1;87(5):1115-34.
- Krishnamurthy G, Menon A, Kannan K, Prakash S, Rajendran A, Philips D. Coronary artery disease and mesenteric artery stenosis-Two sides of the same coin?-Long term prospective analysis. Intractable & rare diseases research. 2019 Nov 30;8(4):245-51.
- Valentine RJ, Martin JD, Myers SI, Rossi MB, Clagett GP. Asymptomatic celiac and superior mesenteric artery stenoses are more prevalent among patients with unsuspected renal artery stenoses. Journal of vascular surgery. 1991 Aug 1;14(2):195-9.
- Wilson DB, Mostafavi K, Craven TE, Ayerdi J, Edwards MS, Hansen KJ. Clinical course of mesenteric artery stenosis in elderly Americans. Archives of internal medicine. 2006 Oct 23;166(19):2095-100.
- Thomas JH, Blake K, Pierce GE, Hermreck AS, Seigel E. The clinical course of asymptomatic mesenteric arterial stenosis. Journal of vascular surgery. 1998 May 1;27(5):840-4.
- Wolf O, Heider P, Heinz M, Weiss W, Berger H, Eckstein HH. Chronic mesenteric ischemia–Surgical and interventional options in therapy. Visceral Medicine. 2006;22(1):36-41.
- Björck M, Koelemay M, Acosta S, Goncalves FB, Kölbel T, Kolkman JJ, Lees T, Lefevre JH, Menyhei G, Oderich G, Kolh P. Editor’s choice–management of the diseases of mesenteric arteries and veins: clinical practice guidelines of the European Society of Vascular Surgery (ESVS). European Journal of Vascular and Endovascular Surgery. 2017 Apr 1;53(4):460-510.
- Cronenwett JL, Johnston KW. Rutherford’s vascular surgery e-book. Elsevier Health Sciences; 2014 Mar 12.
- Oderich GS, Bower TC, Sullivan TM, Bjarnason H, Cha S, Gloviczki P. Open versus endovascular revascularization for chronic mesenteric ischemia: risk-stratified outcomes. Journal of vascular surgery. 2009 Jun 1;49(6):1472-9.

Fig 1: Well collateralised abdominal mesenteric vasculature showing the arc of buhler and arc of drummond.

Fig 2: Stenosis of coeliac ostium with post stenotic dilatation, short segment 2.5 cms occlusion of SMA and severely diseased abdominal aortic wall.
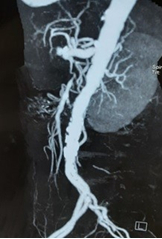
Fig 3: Pale bowel loops and thinned out SMA reforming from middle colic artery (left), ileo-mesenteric (SMA) bypass with 6×20 Goretex graft
 Dr. Sugi Subramaniam
Dr. Sugi Subramaniam
Consultant, Liver Transplant and HPB Surgery
Kauvery Hospital