
Abstract:
Severe hyperkalemia is a potentially life threatening cardiac emergency, especially in patients with renal failure, which can lead to fatal arrhythmias such as ventricular tachycardia (pulseless), ventricular fibrillation or even asystole, leading to cardiac arrest. VT Storm a rare electrical phenomenon that is life threatening and involves recurrent episodes of ventricular arrhythmias. We discuss in our case report, a 72 years gentleman, with recurrent severe hyperkalemia, recurrent cardiac arrest and VT storm.
Key words:
Hyperkalemia, kidney failure, cardiac arrest, emergency hemodialysis, VT Storm
Case history:
72 years gentleman, a known Hypertensive, CAD- Post CABG with severe LV dysfunction (2006), IABP with Complex PCI (2020), S/P ICD implanted for multiple NSVT (2020), CKD stage V on HD (3/7), Dyslipidaemia, left radiocephalic AV fistula with left innominate vein thrombus with narrowing on oral anticoagulants, presented to ER on 5.6.2022 at around 10.45pm with H/O sudden onset chest discomfort associated with burping for past 1 hour
He also gave history of shortness of breath – grade 3 NYHA since evening.
No H/O giddiness, LOC, palpitation, sweating, orthopnoea, abdominal pain, vomiting, loose stools, fever, cough, cold.
Last Hemodialysis was done on 4th June 2022
On initial evaluation at ED
Airway
Patent, self-maintained. C-spine clinically cleared.
Breathing
RR – 24/ min, mildly tachypnoeic
Spo2 – 99% RA, B/L air entry equal, B/L fine basal creps.
Circulation
BP – 150/100, HR – 100/ min,
CVS – S1S2 normal, no murmur, JVP – Prominent, cold and clammy peripheries,
peripheral pulses feebly felt.
PA – Soft, non-tender, no organomegaly and bowel sounds heard.
Disability
GCS – E4V5M6 [15/ 15]
B/L pupils equally reacting to light 3mm
Moving all 4 limbs
CBG – 189mg/dl
Exposure
AV fistula present on left Upper limb
Implantable Cardiac Defibrillator insitu
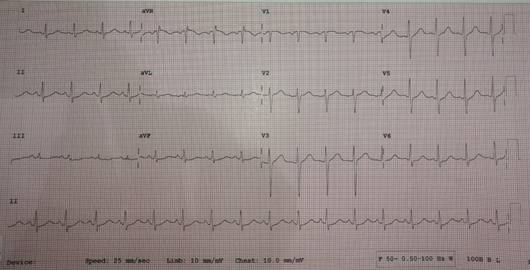
Initial ECG – showed Sine wave pattern
CHEM – 8
Na + – 141 mmol/ L
K + – 7.6 mmol / L
Cl – – 112 mmol/ L
GLU – 192 mg/ dl
BUN – 75 mg/ dl
CREAT – 13.2 mg/ dl
HCT – 27.9% PCV
HB – 8.8 g/ dl
TROP-I: 0.185 (positive) – post cardiac arrest reverted state
ECHO: ICD implant & pacemaker lead insitu, mild global hypokinesia with regional variation and mild LV dysfucntion with EF-45%, Moderate PAH, Significant LVH, dilated LA, RA & LV, grade II MR & grade II TR.
MANAGEMENT IN ER:
Patient was put on propped position and quickly 2 wide bore intravenous cannula secured. In view of severe hyperkalemia with significant ECG changes – sine wave pattern and a potassium of 7.6 mmol/l, hyperkalemia correction was given with 1) 10% calcium gluconate 30ml was administered iv over 10-15mins, 2) Human Actrapid 8units in 25% dextrose 100ml infusion given over 20mis, and 3) Asthalin nebulization 10mg P/N given as stat dose.
Patient’s condition was discussed with the nephrologist and was planned for emergency hemodialysis.
Around 11.40 pm, when patient was about to be shifted to intensive care unit, patient went into sudden cardiac arrest, monitor showing pulseless ventricular tachycardia and hence immediately CPR was commenced as per ACLS protocol and DC shock 200 J was delivered. After obtaining informed consent from the attenders, airway was secured with 8 size ET tube at lip level 21, confirming the position by 5 point auscultation.
Again considering severe refractory hyperkalemia as the cause of pulseless Ventricular tachycardia, another hyperkalemia correction dose was given which included 30ml of 10% calcium gluconate as iv bolus, Human Actrapid 8 units in 25% dextrose 100ml iv bolus was given and was CPR continued.
Patient continued to have recurrent pulseless VT and hence multiple shocks were delivered.
Around 12.10 am, ROSC obtained for few seconds and patient went into PEA again.
After prolonged CPR of 45 mins, finally ROSC obtained at around 12.25am,
Patient was started on Adrenaline infusion @10ml/hr.
Post ROSC vitals: BP – 160/100 mm Hg
HR – 102/min
SpO2 – 96%
Repeat ECG – showing LBBB pattern
Repeat ABG showed severe metabolic acidosis with pH 7.03 and HCO3 14.1
After discussing with the family, patient was started on CRRT (through right IJV HD catheter) due to hemodynamic instability. He was initially on ventilator and then later extubated on 6/6/2002 evening.
Repeat ECG was normal. Serum potassium was 5.30 (7/6/2022) and 4.89 (8/6/2022). Cardiologist opinion was obtained. His overall poor prognosis with ICD implant and recurrent chance of cardiac arrest on HD, option of peritoneal dialysis as an alternate to HD as there is hemodynamic compromise was explained to the attender in detail. Patient was then discharged in a stable condition without any neurological deficit on 9/6/2022.
Subsequently, on follow up, patient developed another episode of cardiac arrest in the dialysis unit 2 weeks later and this time the implantable cardiac defibrillator was functioning aversed to the previous time when the machine failed to shock the patient. This episode the ICD delivered shocks along side CPR, and an expert electrophysiologist opinion was sorted and patient underwent electrophysiological studies and RF ablation for the recurrent VT storm post ROSC and now he is doing well and continues to come for routine hemodialysis 3 times a week.
Discussion:
Hyperkalemia:
Emergency departments frequently admit cases of hyperkalemia, a common electrolyte disorder. Among the typical underlying predisposing conditions are heart failure, diabetes mellitus, significant tissue trauma and moderate to severe kidney disease. Medications such as nonsteroidal anti-inflammatory drugs, succinylcholine, digitalis, potassium-sparing diuretics and inhibitors of the renin-angiotensin-aldosterone systemare frequently associated with hyperkalemia.
Symptoms and consequences of hyperkalemia
While many patients are asymptomatic, hyperkalemia may manifest clinically by muscle weakness. Paresthesias and muscular fasciculations in the arms and legs might be earlier signs of hyperkalemia. Paralysis, cardiac conduction abnormalities, and cardiac arrhythmias can be lethal.
Stages:
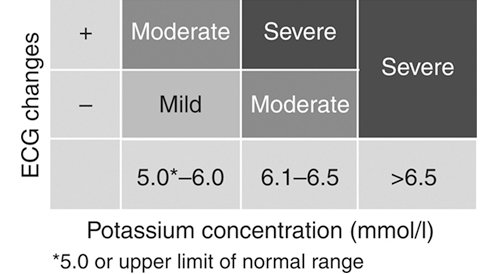
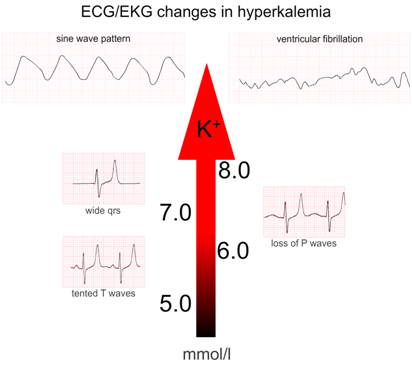
ECG Changes:
Treatment of Hyperkalemia:
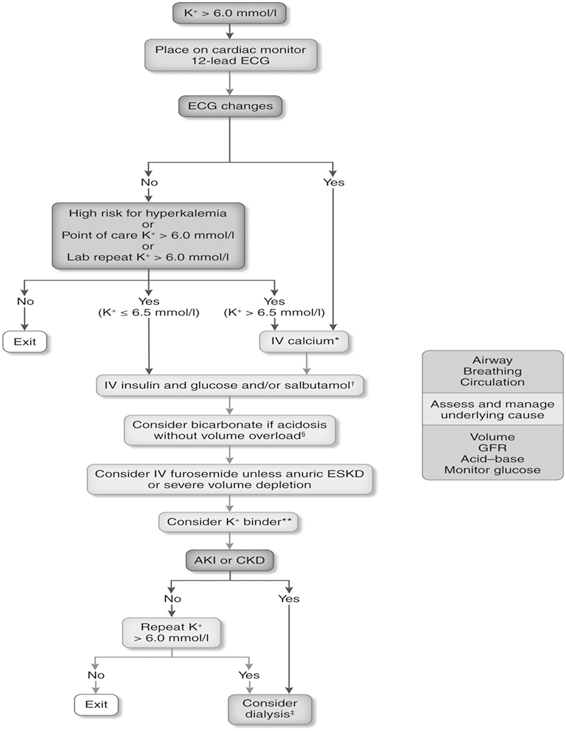
Treatment algorithm for management of acute hyperkalemia in the emergency department(3)
- Inj calcium gulconate 10% 10 ml over 5 min , can be repeated 3 times, in order to stabilize the mocardium
- Injection human insulin ( short acting insulin) 10 units in 50 ml of 50% dextrose over 10-20 mins to shift potassium back into the cells.
- 20 ml ie 10 mg of nubilsed salbutamol can be given over 10-20 min to push potassium back into the cells
- IV bicarbonate & potassium binders can be considered where there is worsening metabolic
- Emergency Haemodialysis is the modality of preference for refractory hyperkalemia with severe metabolic acidosis
Ventricular tachycardia or Ventricular fibrillation (Electrical Storm) & Implantable cardiac defibrillator:
An electrical storm is a life threatening condition that results in repeated episodes of ventricular arrhythmias. The definition of this condition is that there are a minimum of 3 sustained episodes of ventricular fibrillation (VF), ventricular tachycardia (VT) or appropriate implantable cardioverter-defibrillator (ICD) shocks that occur during a 24 hour period. A situation of sustained VT is one that lasts for 30 seconds and requires hemodynamic compromise or which involves termination of the episode by intervention.
Because the management of electrical storms is a challenge, an approach that is tailored to the underlying cause is essential. The acute phase of myocardial infarctions (MI), inherited arrhythmic syndromes and structural heart disease (an ICD) are the conditions where electrical storms often manifest themselves. Syncope, dizziness and palpitations are among the major symptoms. The clinical presentation may involve multiple episodes of arrhythmias which could be potentially fatal or cardiac arrest. Recurrent shocks frequently present in patients with ICD.A knowledge of arrhythmia conditions, ICD programming, therapeutic options and emerging techniques for the treatment of refractory cases is required for the effective management of hyperkalemia. An organized approach is vital for the effective evaluation and treatment of electrical storms.
Incidence:
Electrical storms occur in 10% to 20% of ICD patients. Those who are experiencing acute MI or have had an MI in the past and those with inherited arrhythmic syndrome are very susceptible to this condition. The incidence of electrical storms varies and depends on the specific populations that are studied.
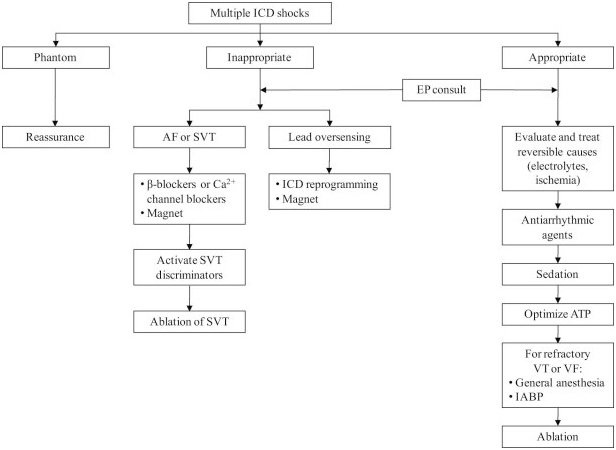
The figure above is an algorithm explaining the etiology of an ICD storm which may result from appropriate therapy (antitachycardia pacing, cardioversion, or defibrillation) and inappropriate therapy (shocks without evidence of an arrhythmia), or phantom shocks. (4)
In cases of ongoing arrhythmia with hemodynamic compromise, the arrhythmia should be corrected immediately & device interogation should be done. Shocks delivered without evidence of an arrhythmia indicate device malfunction. In all these situations, coordination with an expert electrophysiologist is important for these patients.
Conclusion:
Recognizing sever hyperkalemia and fatal cardiac arrhythmias with immediate, prompt and aggressive treatment towards correction of imbalance helps in reducing risk of cardaic arrest.
Electrical storm, an increasingly common life threatening situation, which needs immediate attention after expert electrophysiologist consultation.
References:
1) Lindner, Gregora; Burdmann, Emmanuel A.b; Clase, Catherine M.c; Hemmelgarn, Brenda R.d; Herzog, Charles A.e; Małyszko, Jolantaf; Nagahama, Masahikog; Pecoits-Filho, Robertoh; Rafique, Zubaidi; Rossignol, Patrickj; Singer, Adam J.k Acute hyperkalemia in the emergency department: a summary from a Kidney Disease: Improving Global Outcomes conference, European Journal of Emergency Medicine: October 2020 – Volume 27 – Issue 5 – p 329-337
2) Robert Buttner and Ed Burns, https://litfl.com/hyperkalaemia-ecg-library/ Mar 24, 2022
- Authors: Andrew Parfitt, Emma Townsend / Editors: Steve Fordham / Reviewer: Chris Gray / Codes: HAP10, NepC1, NepC2, NepC3, NepC5, NepP1, SLO1 /co.uk/Published: 16/09/2019
- Eifling M, Razavi M, Massumi A. The evaluation and management of electrical storm. Tex Heart Inst J. 2011;38(2):111-21. PMID: 21494516; PMCID: PMC3066819.
 Dr. T. Niveanthini Arun
Dr. T. Niveanthini Arun Dr. Aslesha Sheth
Dr. Aslesha Sheth
{kind=link}