Abstract:
We report a 72-year-old male who came to the emergency department with fever, altered sensorium, neck rigidity and new onset seizures, features suggestive of meningitis. MRI brain showed a cerebritis with subarachnoid hemorrhage (SAH). Patient was also found to have low blood counts and was suspected to have myelodysplastic picture. Blood cultures grew Bacillus cereus for which patient was treated with vancomycin, meropenem, fluconazole and patient recovered. We have chosen to report this case because Bacillus cereus presenting with subarachnoid haemorrhage and neutropenic sepsis is rare.
Case report:
A 72-year-old male presented to the emergency department of Kauvery hospital with the history of low-grade fever for one day and severe headache in the occipital region with neck pain, following which he developed 2 episodes of GTCS within few hours. On arrival the patient was in post ictal state. His vitals are as listed in (table1). Patient’s saturation in room air was only 84% and his airway was threatened so oropharyngeal airway was inserted and saturation increased to 95% with 5 litres of O2.

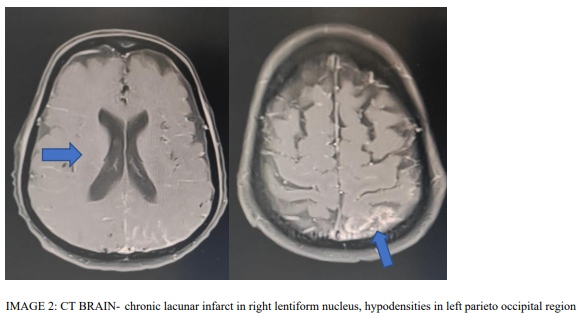
Based on the clinical information, intracerebral bleed was suspected, hence patient was shifted to CT BRAIN which showed small Subarachanoid hemorrhage SAH in the parietal concavity (IMAGE 2).
Blood reports showed WBC of 400 and platelets of 20000. Liver parameters were deranged and there was a prerenal azotemia. Electrolytes and Arterial blood gas analysis were normal. CSF analysis was done (TABLE 2).

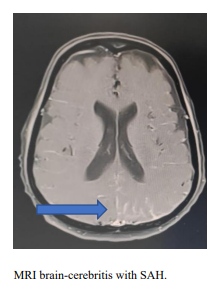
In context of severe leukopenia, multiorgan dysfunction, with prolonged altered sensorium, low grade fever, this small SAH was not adequate to explain the patient’s clinical status. We suspected a systemic sepsis with meningoencephalitis and proceeded with MRI of Brain with contrast study.
MRI brain showed focal cerebritis in left parietal cortex with leptomeningeal enhancement out of proportion to the SAH confirming our clinical suspicion of an infective meningitis (IMAGE1)
In this setting of SAH with leptomeningitis and cerebritis and a past history of invasive aspergilloma with immunocompromised state we suspected a fungal sepsis with seeding in the meninges causing bleed and infection. We also suspected a infective endocarditis which was ruled out with a ECHO. Blood and urine cultures were sent and he was started on Vancomycin, Meropenam and fluconazole in meningitis dose. He was also treated with antiepileptics. He was started on Colony stimulating factor and was transfused with 2 units of packed red blood cells and 6 units of Random donor platelets during his course in hospital. He was on Non-invasive ventilation at the time of admission. Blood culture revealed bacillus cereus. We reconfirmed the growth again as bacillus cereus as it is a rare organism to cause sepsis. A diagnosis of Bacillus cereus sepsis with Focal cerebritis with leptomeningitis and SAH was made on day 5. Meropenam and flucanozole was stopped. His blood parameters improved with resolution of infection. CSF analysis was done after platelets improved > 50000. CSF was xanthochromic and inflamatory(TABLE 3). No organism grew in the CSF. He improved clinically to room air but contracted a hospital acquired pneumonia. He was started on polymyxin for this infection. He made a good recovery after a 14-day course of Vancomycin and 1 week of polymyxin patient was discharged in room air.
IMAGE 1:
A diagnosis BACILLUS CEREUS NEUTROPENIC MENINGITIS WITH SAH was made.
After receiving IV antiepileptics, IV antibiotics, blood transfusions and GCSF injections, patient showed recovery after 6 days. Patient was reviewed after one week and found to be stable.
Discussion:
Bacillus cereus as an organism is known to cause gastrointestinal problems.
Bacillus is a spore forming gram-positive rod-shaped bacterium that is ubiquitous in environment. It is one of the rare causes on meningitis. Bacillus cereus is regarded as opportunistic pathogen. It produces enterotoxi, emetic toxin, hemolysin, phospholipase C, beta lactamases, protease, and collagens.
The S layer has a significant role in adhesion to host cells and in phagocytosis[1] our patient presented with gastrointestinal manifestations but due to his immunocompromised state, the organism entered the blood stream and caused sepsis and meningitis.
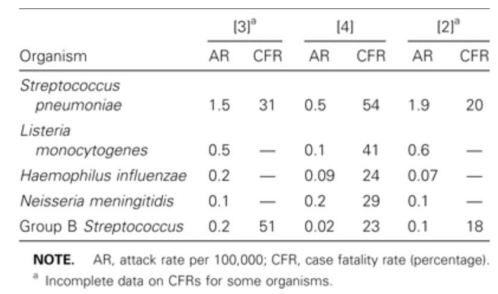
Organisms causing meningitis in elderly:
Data from surveillance studies of bacterial meningitis in older adults (aged >60 years).[2]
Most common fungal infections causing meningitis: [3] Candidiasis, Cryptococcus, Aspergillus, zygomycetes
In a study done between April 2000 and may 2005 in a hematology unit in Turkey, 350 bacteremia episodes occurred. Most common were gram positive pathogens (228 cases) especially coagulate negative staphylococci and staphylococcus aureus, of that Bacillus cereus accounted for 3.4% [4]
The proportion of patients with nosocomial blood stream infection who have an underlying malignancy is 10% based on surveillance and control of pathogens of epidemologic importance [SCOPE]
Gram positive organisms were observed in 76% and gram negative organism accounted for 14%. Neutropenia was observed in 13% of patients. The crude mortality was 31 % for non neutropenic patients.[5]
The most common source points are
- Central venous catheters
- Gastrointestinal manifestations
Poor prognostic features in Bacillus cereus infections:[6]
- Deranged liver function tests
- Neurological involvement
- Neutropenia
Bacillus cereus was also commonly seen in patients with hematologic malignancies who were receiving chemotherapy due to break in mucosal barrier. However, prophylaxis with quinolones on patients diagnosed of leukaemia and receiving chemotherapy did not report any Bacillus cereus growth.[7].
In a series of 13 cases of B. cereus septicemia occurring in patients with hematological disease, four died of infection and nine fully recovered, thus resulting in a 31% mortality rate.[7]
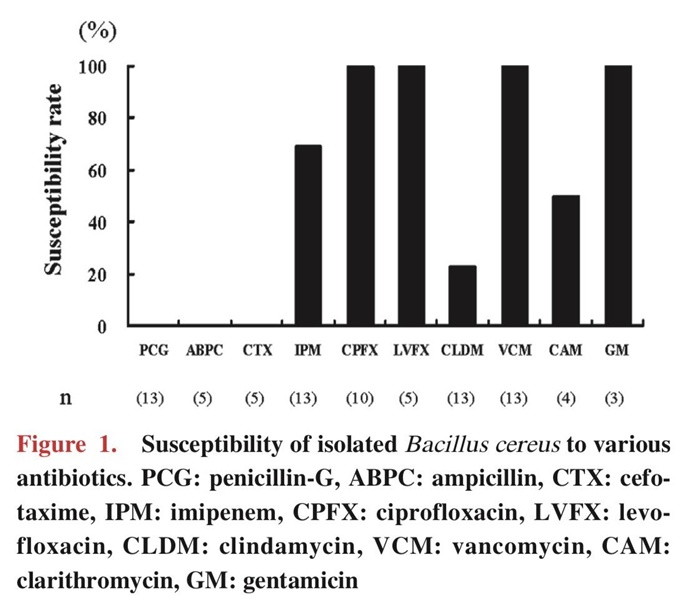
The optimal antibiotic for treatment of Bacillus cereus were vancomycin, and quinolones. http://www. Clsi.org suggested resistance to carbapenem and Clindamycin.[7]
Since the patient was started on antibiotic therapy as early as in the emergency room, despite have elevated liver function tests and neutropenia and subarachnoid haemorrhage, the patient’s prognosis gradually improved and was eventually discharged
Conclusion:
Take Home points
- To maintain high index of suspicion of Bacillus cereus infection in patient with neutropenic sepsis, meningitis, SAH. With earlier treatment the outcome is better
- Bacillus cereus is one of the common infections in haematologic malignancy patients but can be prevented by prophylactic treatment with fluroquinolones
- Following strict aseptic precautions during IV catheterisation will prevent Bacillus cereus growth and remains the gold standard
Review of literature:
- Epidemiology and pathogenesis of Bacillus cereus Anja Kotiranta et al
- Bacterial Meningitis in Aging Adults Chester Choi Clinical Infectious Diseases, Volume 33, Issue 8, 15 October 2001, Pages 1380–1385
- Fungal CNS infections in patients with hematologic malignancy Livio Pagano, Morena Caira, Paolo Falcucci& Luana Fianchi Pages 775-785 | Published online: 10 Jan 2014
- A Case Series of Bacillus Cereus Septicemia in Patients with Hematological Disease (Intern Med 51: 2733-2738, 2012) (DOI:10.2169/internalmedicine.51.7258)
- Bacillus spp. among hospitalized patients with haematological malignancies: clinical features, epidemics and outcomes V. Ozkocaman et all
- Fulminant sepsis caused by Bacillus cereus in patients with hematologic malignancies: analysis of its prognosis and risk Daichi Inoue et al
- Current trends in the epidemiology of nosocomial bloodstream infections in patients with hematological malignancies and solid neoplasms in hospitals in the United States Hilmar Wisplinghoff 1, Harald Seifert, Richard P Wenzel, Michael B Edmond PMID: 1271530 DOI: 10.1086/374339
 Dr.M karthi
Dr.M karthi
PG Resident
Kauvery Hospital