A 57-year-old male patient presented to our radiology department with complaints of pain during prolong sitting or during defecation. An outside MRI report indicated coccydynia with a posterior spicule spur and degenerative changes in the sacrococcygeal joint.
Along with orthopaedic department, we decided to perform a CT-guided ganglion impar block due to the failed conservative management. During the procedure, the patient was positioned prone on the CT gantry, with their hips slightly flexed by placing a pillow beneath their abdomen and their legs internally rotated. Under aseptic precaution, under CT guidance using a lateral approach, 22 G needle was inserted laterally, thereby reaching the precoccygeal space. This lateral approach was employed to minimize the risk of rectal perforation and faecal contamination. The needle was directed towards the ganglion impar, which is located at or just below the sacrococcygeal joint.
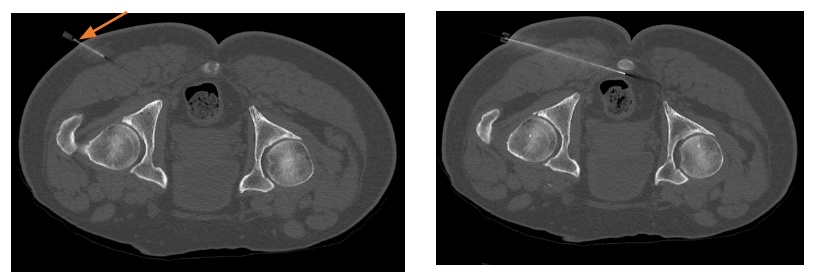
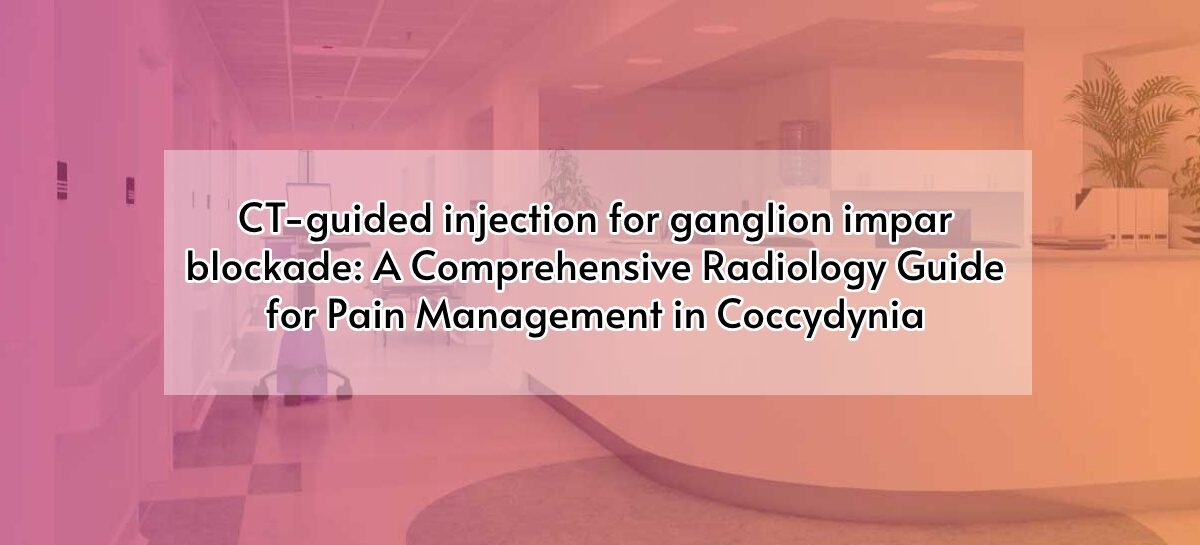
Axial sections of CT bony pelvis A) show entry site of needle (arrow) in right gluteus approximately 6-9 cm from the midline. B) The needle reached the target site.
Once the needle reached its target, location of the needle tip is confirmed with injection of a small amount of non-ionic contrast material. After confirmation, a mixture of 40 mg of triamcinolone and 2 mL of 2%lignocaine is injected. Then check CT was performed to look for any rectal perforation and faecal contamination.
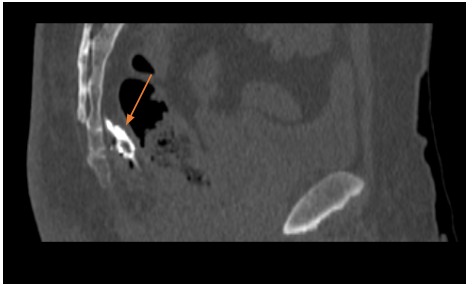

Axial and sagittal sections of bony pelvis showed the injection of contrast (arrow) to confirm the location
Discussion:
The ganglion impar, also known as the ganglion of Walther, is the final point of convergence for the pelvic sympathetic chain, situated in front of the coccyx. It is responsible for transmitting sympathetic efferents and nociceptive afferents to and from the perineum, distal rectum, distal vagina, distal urethra, and anus.
Coccydynia, characterized by pain in the coccyx or tailbone region. Common etiologies include trauma (e.g., falls or childbirth-related injury), degenerative changes (e.g., coccygeal spurs or disc degeneration),inflammation (e.g., coccygeal bursitis), and rare causes such as tumors or infections.
Conservative treatment consists of physiotherapy, exercises, and pain management with oral analgesics and use of a coccyx pillow while sitting.
Interventional approaches are considered when conventional treatments fail to alleviate coccydynia. These procedures, such as coccygeal injections, ganglion impar blocks, or radiofrequency ablation, aim to target specific pain sources and decrease inflammation, thereby providing symptomatic relief.
Surgical intervention may be pondered for certain cases involving structural abnormalities, chronic pain, or unstable traumatic fractures. Coccygectomy, which entails partial or complete removal of the coccyx by experienced surgeons, is a surgical option aimed at mitigating pain and improving overall quality of life.
To summarize, CT-guided injections for the sacro-coccygeal region offer several benefits over fluoroscopy-guided injections. These advantages include a high level of confidence in accurate needle placement, a more straightforward approach to covering a wide area, a reduced risk of complications due to unintended injections into major pelvic structures, and a higher probability of reaching the ganglion impar, particularly in cases where the ganglion impar’s location varies anatomically.
 Dr Kanagasabai Kamalasekar
Dr Kanagasabai Kamalasekar Dr. Vijay Thiraviyam
Dr. Vijay Thiraviyam Dr. Firdhous Begum
Dr. Firdhous Begum
{kind=link}