INTRODUCTION:
Monitored anaesthesia care is a specific anaesthesia technique for therapeutic and diagnostic procedure done under local anaesthesia along with sedation and analgesia titrated to a level that preserve spontaneous breathing and airway reflex, it has three basic components – a safe conscious sedation, measure to allay patient’s anxiety and effective pain control.
It has less physiological disturbance and more rapid recovery than general anaesthesia. Sedation ranges from minimum to moderate (patient remain asleep but easily arousable) to deep sedation (patient can be aroused only by painful stimuli).
Sub dural haemotoma is collection of blood in subdural space due to bleeding of bridging veins that traverse the dural cell layer of dural border. Common causes of SDH are trauma, elderly, antithrombotic medication, alcohol and iatrogenic. Clinical features include decreased GCS, headache, seizures, instability and disorientation. Treatment for SDH is surgical evacuation – burr hole evacuation.
INJ.REMIFENTANIL:
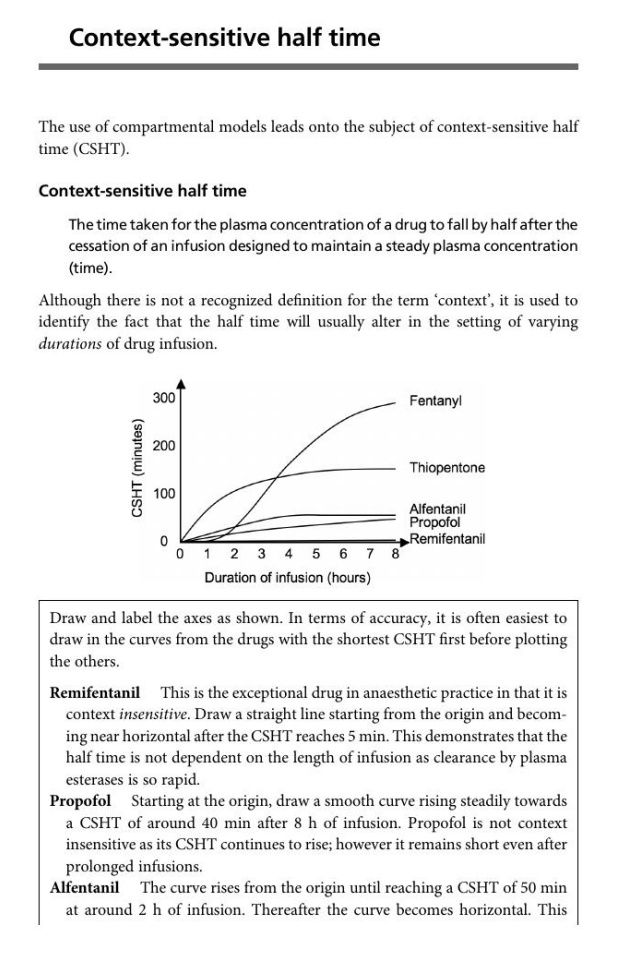
Inj.Remifentanil is a ultra short acting synthetic opioids introduced in 1997 which is 2000 times more potent than morphine. Adult doses – 1 mcg/kg body weight. Continuous infusion rate – 0.05 mcg/kg/min. Two major pharmacokinetics effects are – very rapid achievement of peak effect and rapid elimination followed by cessation of the effect within five minutes after discontinuing the infusion. Rapidly metabolized by non-specific plasma and tissue esterase to remifentanil acid and excreted. Hepatic and renal dysfunction has no effect on clearance. Context sensitive half time for remifentanil is 3 minutes even after hours of infusion. Context sensitive half time is a time taken for blood plasma concentration of a drug to decline by one half after an infusion design to maintain steady plasma state. TCI (Target Controlled Infusion) pump used for remifentanil infusion – computer control infusion method which deliver anaesthetic drug based on patient height, weight, age and gender to achieve (CeT) effect site concentration. Side effects of remifentanil are respiratory depression, urinary retention, hypotension, bradycardia, stimulate vasovagal response and PONV.
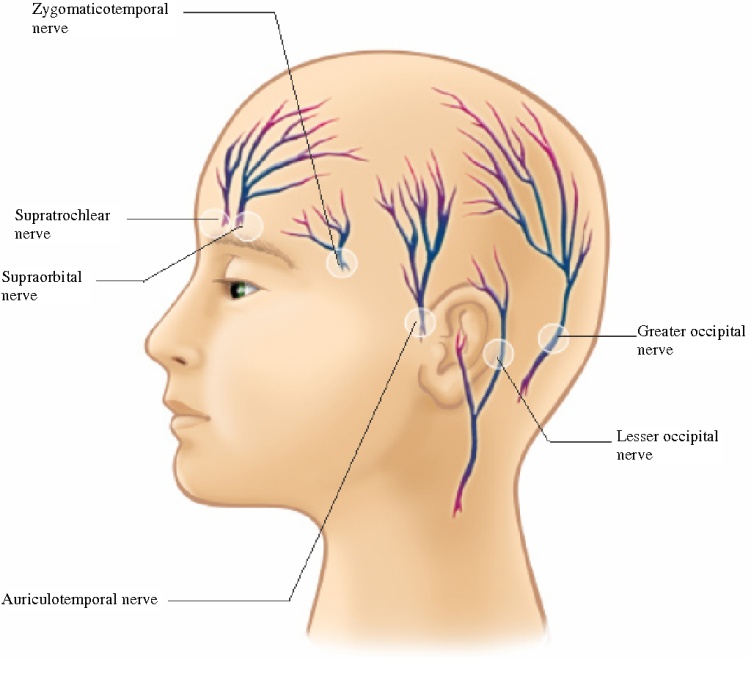
Coming to scalp block, where Local anaesthetict drug is injected in to 6 nerves bilateral. Nerves to be blocked are supra orbital nerve, supra trochlear nerve, auriculotemporal nerve, zygomaticotemporal nerve, greater occipital nerve and lesser occipital nerve.
CASE SCENARIO:
A 73 years old gentleman, ASA 3 with known case of hypertension and CAD -TVD, post PTCA(2020) status had history of seizure of 2 min (tonic clonic )Episode one month back, Brain imaging done, CT brain showed chronic SDH of 5×4 cm, planned for burr hole evacuation, patient and attenders explained the procedure, patient deferred the surgery, started on antiepileptics, lately now presented to ER with headache. Proceeded to Burr hole under scalp block and Inj.remifentanil infusion.
- PREOP: Pre-anaesthetic checkup done.
Routine investigation including complete blood count, renal function test, liver function test, coagulation profile, ECG, chest x ray and echo done, Labs wnl, except echo- EF: 45%,Severe aortic stenosis of valve area : 0.9cm 2,severe pah -61mmhg,rwma +. Cardiologist clearance under high risk. Airway assesed, MP 3,With good mouth opening.
Attenders and patient prognosticated and plan of anaesthesia with high risk explained .
Npo orders given, premedication advised, antiplatelet stopped as per guidelines.
INRAOP:
IV access secured, monitors attached, face mask oxygen connected with Etco2, initial vitals recorded and found to be within normal limits, ETCO2 good trace obtained.
Remifentanil infusion started in TCI pump (minto), after entering patient details,. Dilution – 2 ml ampule diluted in 40 ml of NS – 50 mcg/ml started at 2 ng/ml. After 120 seconds patient become moderately sedated according to RAAS score minus 2.
Scalp block was given with 0.75 % ropivacaine 40 ml diluted with 40 ml NS and given to all six nerves bilaterally, pain assessed in scalp after block with pin prick test – patient was pain free.
Horseshoe head was fixed and procedure started, at the time of incision remifentanil dose increased to 3 ng/ml, initial vitals showed mild hypotension settled with vasopressors, airway maintained with good Etco2 trace.
Surgery was uneventful, at the time of dressing remifentanil infusion stopped, patient become fully awake after 5 minutes of stopping Remifentanil.
Patient shifted to recovery, vitals stable, GCS 15/15, VAS 2/10.
CONCLUSION:
So, to conclude ,in our case – for monitored anaesthesia care, for minimal invasive procedures, for high risk patient, Inj.Remifentanil has done a good job in maintaining patient haemodynamics,mild sedation, with analgesic action, with aireay patent – by achieving effect site concentration within minutes and reversing of the same actions, immediate post-surgery. Scalp block has added its own benefit in providing painless scalp area with minimal oozing.
Therefore Inj.Remifentanil will overcome all the other opiods side effects ,with maximum benefits ,and lesser haemodynamic changes.
 Dr. R.B. Gurulakshmi
Dr. R.B. Gurulakshmi
Final Year Postgraduate
Diploma in Anaesthesia
Kauvery Hospital, Chennai
Mentors:
 Dr. Velmurugan Deisingh
Dr. Velmurugan Deisingh
M.B.B.S., D.A., D.N.B.(Anesthesiology)
Senior Consultant
Kauvery Hospital, Chennai

Dr. Jamila Khatoon
MBBS, DNB Anesthesia
Junior Consultant
Kauvery Hospital, Chennai