
57-year-old post-menopausal female came to our radiology department, Kauvery hospital, Alwarpet, Chennai with complaints of lower abdominal pain.
No prior imaging is available for comparison. MRI pelvis showed thickened and homogeneously hypointense fibrous cortex with mild delayed peripheral enhancement seen in both ovaries
This article highlights the MRI features to distinguish the ovarian fibromatosis with ovarian fibroma.
Introduction:
Ovarian fibromatosis is a rare, benign, non-neoplastic condition characterized by the enlargement of the ovaries due to fibrosis of the ovarian stroma. While it can occur at any age, it is most commonly observed in younger patients, with an average age of onset around 25 years (1). Patients may be asymptomatic or experience symptoms such as abdominal pain, menstrual irregularities, and, in some cases, hirsutism or virilization (2).
Case report:
57 years old post menopausal female came to our radiology department. No complaints of post-menopausal bleeding. No other comorbidities.
MRI pelvis was taken in 1.5T MRI machine. There is lobulated, heterogeneously appearing structures in bilateral adnexa measuring about 4.6 x 2.6 x 2.3 cm on the right and 4.3 x 3.4 x 2.5 cm on the left side – likely representing enlarged ovaries. It shows thickened and homogeneously hypointense T1w/T2w periphery (maximum thickness of about 10 mm) – likely representing thickened and fibrous cortex ( likely MR Black garland sign)
The central aspect appears isointense on T1w and heterogeneously hyperintense on T2w No suppression on fat saturated images to indicate fat component within. No evidence of restricted diffusion. Subtle blooming on SWI images on the right side.
Post-contrast image shows mild delayed enhancement. Mild free fluid in the pouch of Douglas.
The absence of significant enhancement during the parenchymal phase of dynamic MR imaging, and the mild enhancement on delayed MR images, were related to the fibrous component of the masses.

FIG 1: MRI T1 axial T2 coronal sections shows thickened and homogeneously hypointense T1w/T2w periphery – likely representing thickened and fibrous cortex ( likely MR Black garland sign).
The central aspect appears isointense on T1w and heterogeneously hyperintense on T2w images.
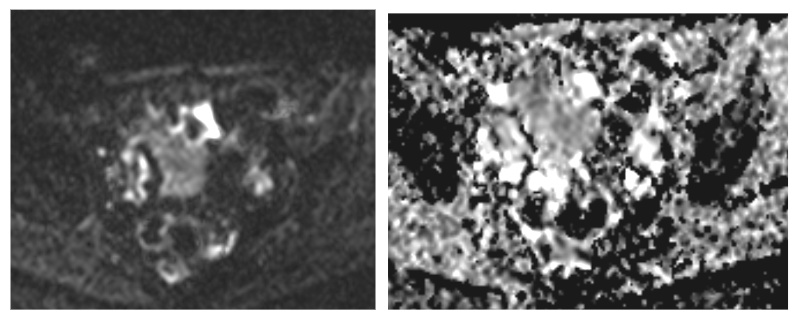
FIG 2: MRI DWI and ADC shows no evidence of restricted diffusion.

FIG 3: A) MRI contrast first phase shows no significant enhancement. B)Delayed phase show mild peripheral enhancement
Pathology:
Histologically, ovarian fibromatosis is characterized by a proliferation of collagen-producing spindle cells surrounding normal ovarian structures causing thickening of the superficial cortex and enlargement of the ovary.
The “black garland” appearance of the cortex with preservation of a normal, central ovarian parenchyma helps distinguish this benign condition from other fibrotic lesions of the ovary, such as fibromas, fibrothecomas or brenner tumors.
Ultrasound:
The echogenicity of ovarian fibromatosis on ultrasound can be variable; preserved ovarian follicles may be seen along the periphery of the mass.
MRI:
T1: hypointense
T2: thick hypointense rim, known as the “black garland sign” (3)
TI c+ Gd: The absence of significant enhancement during the parenchymal phase of dynamic MR imaging, and the mild enhancement on delayed MR images, were related to the fibrous component of the masses.
Differential diagnosis
Ovarian fibroma
MRI
T1: usually demonstrate homogeneous low signal intensity
T2:Appear as well-circumscribed masses with low signal intensity.
T1 C+ (Gd): usually shows heterogeneous enhancement
Ovarian fibrothecoma
MRI
T1: typically shows homogeneous low signal intensity
T2 :Lesions show predominantly homogeneous low signal intensity (from fibrous components)
scattered high signal areas may be present, representing areas of cystic degeneration +/- oedema
Brenner tumour
CT-Calcifications have been reported in ~85% of Brenner tumours on CT. The solid component may show mild to moderate enhancement post-contrast
MRI -Due to its predominantly fibrous content, they appear hypointense on T2-weighted sequence
Thecoma
MRI T2 –usually hyperintense (often from oedema and cystic degeneration), but may be variable
may mimic more common malignant ovarian tumours
In phase-Opposed phase: intratumoural lipid may give a chemical shift artifact 3.
Conclusion:
It is observed that fibromatosis of the ovary is not a well-recognized entity and many clinicians are not aware of its existence. It is, therefore, often misdiagnosed as a malignant ovarian tumor, and more extensive treatment than is necessary is undertaken. Ovarian fibromas and fibrothecomas occur at all ages, but most frequently during the fifth or sixth decade of life, and are often unilateral and asymptomatic.
In conclusion, ovarian fibromatosis should be considered in women with solid ovarian tumors that have a predominant fibrous component. The presence of ovarian infiltration, with partial sparing of normal ovarian structures, which is particularly visible on MR imaging, can help to distinguish fibromatosis from ovarian fibroma. Accurate diagnosis is essential to avoid radical surgery, especially since most of the patients are young females.
References
- Bazot M, Salem C, Cortez A, Antoine JM, Daraï E. Imaging of ovarian fibromatosis. American Journal of Roentgenology. 2003 May;180(5):1288-90.
- Lalwani N, Patel S, Ha KY, Shanbhogue AK, Nagar AM, Chintapalli KN, Prasad SR. Miscellaneous tumour-like lesions of the ovary: cross-sectional imaging review. The British journal of radiology. 2012 May 1;85(1013):477-86.
- Takeuchi M, Matsuzaki K, Sano N, Furumoto H, Nishitani H. Ovarian fibromatosis: magnetic resonance imaging findings with pathologic correlation. Journal of computer assisted tomography. 2008 Sep 1;32(5):776-7.
 Dr Kanagasabai Kamalasekar
Dr Kanagasabai Kamalasekar
Consultant Radiology
Kauvery Hospital, Chennai
 Dr. Firdhous Begum
Dr. Firdhous Begum
Post Graduate Resident – Radiology
Kauvery Hospital, Chennai

{kind=link}