
ABSTRACT:
Bochdalek hernia is one of two forms of a congenital diaphragmatic hernia, the other form being Morgagni hernia. A Bochdalek hernia in which an opening exists in the infant’s diaphragm, allowing normally intraabdominal organs( particularly the stomach and intestines) to enter into the thoracic cavity. In the majority of people the affected lung will be deformed and the resulting lung compression can be life threatening. Bochdalek hernias occur more commonly on the posterior left side( 85%, versus right side 15%). Bochdalek hernia is more common in neonate and rarely seen in paediatric and adult group. Life threatening complications may develop in asymptomatic patients over time. Surgical treatment is essential upon diagnosis. Following is a rare presentation of diaphragmatic hernia with volvulus in a 10-year-old child who was apparently alright until now
CASE HISTORY:
A 10-year-old girl was brought to ER by parents with C/O abdominal pain associated with nausea & vomiting one episode, non-bilious, non-blood stained for past 2hrs
H/O similar complaints 1 week back and resolved on its own. Her last bowel movement in the morning was not blood stained. No H/o fever, chest pain, SOB, burning micturition, hematamesis, bleeding per rectum.
Birth H/o : Normal delivery , birth weight -2.75 kg
Skipped vaccination from 1.5 years
ON EXAMINATION:
child alert , active , afebrile, wt- 40kg, pain score 4/10
Airway: Patent
Breathing: left side basal air entry decreased,RR-26bpm, SPO2 98% RA
CVS– S1S2 heard no murmur, BP 110/70mmhg
PA: Soft, BS+, mild tenderness over left hypochondric region
CNS : NFND, GCS 15/15
GENITALS- Normal
Initially child was managed symptomatically
On reassessment her symptoms persisted, in view of above clinical presentation chest X-ray done.
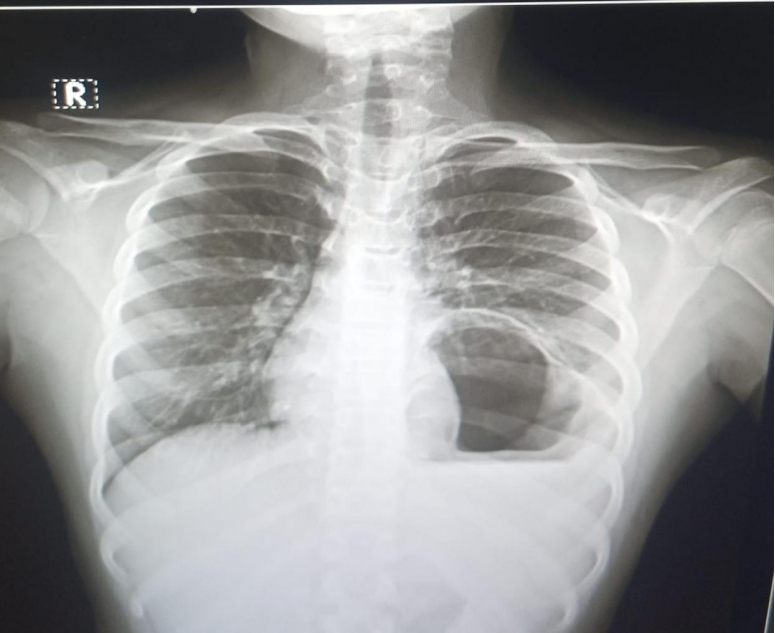
Figure 1. xray chest with gastric bubble in left chest
- CT ABDOMEN showed -OG junction and pylorus of the stomach are intra thoracic, Body of the stomach intrathoracic s/o diaphragmatic hernia.
PROCEDURE:
From the above presentation and investigations child was diagnosed with DIAPHRAGMATIC HERNIA A/K/A BOCHDALEK HERNIA WITH GASTRIC VOLVULUS.
child was taken up for surgery- LAPROSCOPIC LEFT BOCHDALEK HERNIA REPAIR done with left ICD placement. Post procedure uneventful. child discharged in stable condition.
DISCUSSION:
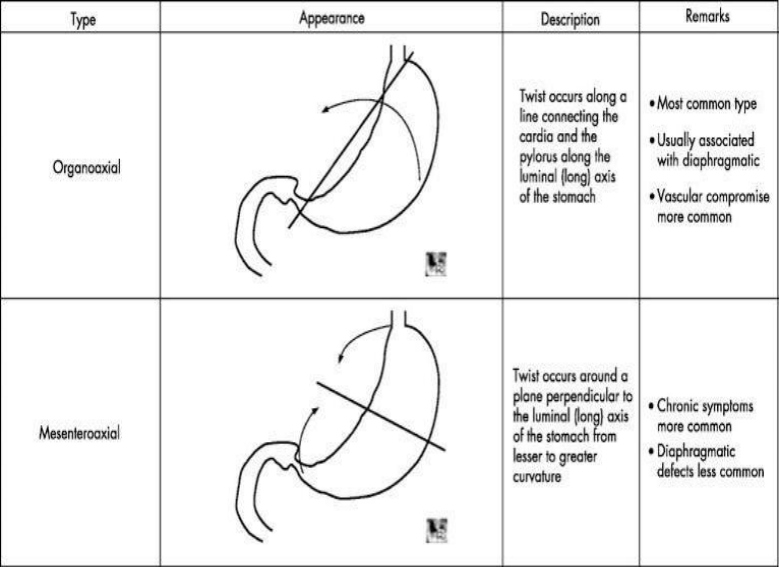
- Gastric volvulus is defined as torsion of more than 180° of the stomach occurring in either the longitudinal, mesenteroaxial, or around both axes.
- Stomach is usually attached to abdominal wall with help of 4 ligaments, gastro phrenic, gastro splenic, gastro colic, gastro hepatic ligaments.
- Acute Gastric volvulus: Borchardt’s triad’, symptoms of nausea and nonprojectile vomiting severe and constant epigastric pain
- There is also difficulty in insertion of nasogastric tube.
TYPES:
- Primary Gastric volvulus is related to an abnormality in the attachment of one among the four gastric ligaments.
- Secondary Gastric volvulus: diaphragmic eventration, carcinoma of the stomach or the pancreas, ulcers, para-oesophageal hernias, abdominal adhesions, or compression of the phrenic nerve
Investigation of choice: Barium swallow
Treatment: Surgical intervention in acute cases.
CONCLUSION:
Bochdalek hernia is a surgical condition primarily diagnosed in infants, typically presents with respiratory symptoms, however, older paediatric and adult presentation without respiratory symptoms have not been documented yet. It is recommended that all diaphragmatic hernia patients undergo surgical repair to prevent incarceration and strangulation of abdominal viscera. In this presentation Mesenteroaxial rotation occurs which is less common than organoaxial. Surgical repair has been associated with low morbidity and mortality and excellent long term outcomes with low rate of recurrence.
REFERENCES:
- Journal of Pediatric Surgery Case Reports 105 (2024) 102821
- Journal of medical case reports
Case reports in gastro enterology
 Dr. Sangavi MC
Dr. Sangavi MC
Emergency Medicine Resident,
Department of Emergency Medicine,
Kauvery Hospital- Alwarpet
 Dr. Ashok Nandagopal
Dr. Ashok Nandagopal
Clinical Lead & Consultant,
Department of Emergency Medicine,
Kauvery Hospital- Alwarpet

{kind=link}