Clinical Details: 37 year male presented with complaints of bilateral gluteal pain for 1 week associated with fever. No history of trauma.
History of difficulty in passing urine, perianal pain on straining at stools (+).
History of fecal incontinence and abdominal distension (+).
Past history of surgery for imperforate anus and appendicectomy.
On examination ,Patient afebrile ,PR – 110/min, BP – 140/90mmHg
P/R – tender from 7 to 9’o’ clock position ; deformed anus, very poor anal tone.
MRI Pelvis revealed:
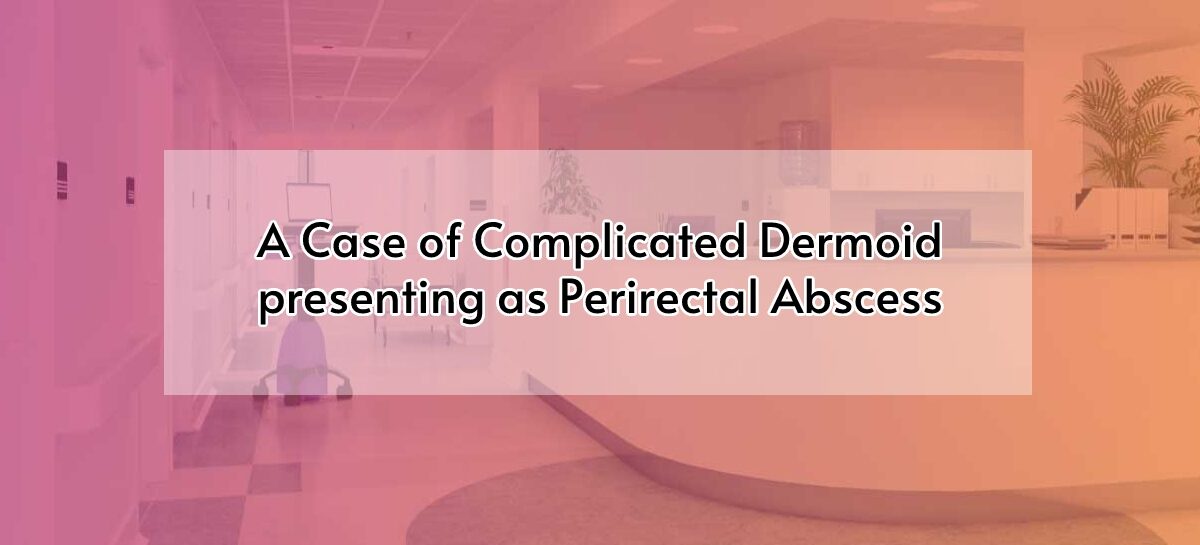
A relatively well capsulated bilobed cystic lesion with internal septations and T1 hyperintense contents in right pelvirectal, ischiorectal and ischioanal fossa, displacing the rectum towards the left side.
The lesion was seen communicating with a right perirectal collection. Peripheral enhancement was noted in the inferior aspect of the lesion.
Perirectal fat stranding and submucosal edema was seen in the anorectum.
The internal and external anal sphincters appeared edematous.

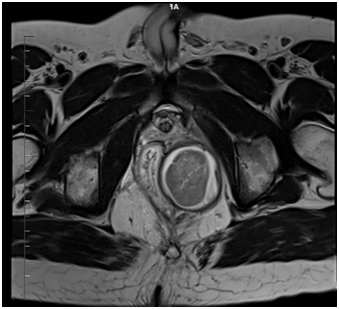
Figure 1a and b – T2W sagittal and axial images showing bilobed hyperintense cystic lesion with internal contents
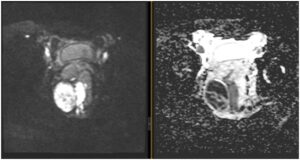
Figure 2 Areas of restricted diffusion within the abscess

Figure 4a and b post contrast T1 axial images shows peripheral enhancement & Perirectal enhancement
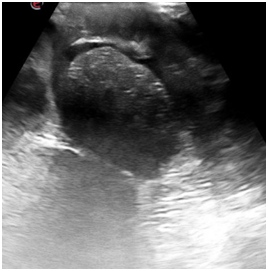
USG imaging revealed well circumscribed heteroechoic lesion with areas of posterior shadowing is seen in perirectal space.
CT imaging revealed areas of hypo-attenuation (fat density) in the lesion

Impression:
Possibility of Dermoid cyst in pelvirectal, ischiorectal and ischioanal fossa with adjoining perirectal abscess (? due to ruptured dermoid).
After anesthetic clearance, with informed consent patient was taken up for surgery. Laparoscopic rectal mobilisation were performed following which laparotomy and drainage of intraabdominal/ perirectal abscess and excision of perirectal dermoid cyst were done. Patient improved symptomatically following the surgery with appropriate clinical care and hence discharged. Patient’s fecal incontinence improved during his post operative period.
Discussion:
Developmental cysts are uncommon cysts with a prevalence of 1 in 40000; they are present from birth and are in the perirectal space. The cysts can be epidermoid, enteric, dermoid and neurenteric cysts. Women in their middle age are the ones usually afflicted with these cysts.
Half the people with developmental cysts do not show any symptoms and the cysts are discovered accidentally during an examination for some other condition. Physical examination of patient may reveal a funnel-shaped dimple in the postanal midline or a long-term perianal fistula. The fistula may be in contact with the cyst.
Big lesions may result in constriction of nearby organs like the rectum and urethra. Constriction of rectum may result in constipation, rectal fullness, pain while passing faeces and tenesmus while constriction of urethra can result in painful urination and frequent urination. In the aggravated form, developmental cysts may result in infection and bleeding. Possibility of malignant degeneration is infrequent.
Dermoid cysts have a border of squamous epithelium and have hair follicles, sweat and sebaceous glands and/or tooth buds.
An ultrasound shows dermoid cysts as unilocular or multilocular lesions with internal echoes as a result of mucus like matter or inflammatory debris.
Imaging with CT reveals unilocular or multilocular hypoattenuating lesions. Co-infections might cause stiffening of the wall of the cyst along with development of inflammation.
Dermoid cysts exhibit increased intensity on T1-WI because of fat content while intensity is of medium range in T2-WI. Keratin debris could be responsible for intralesional foci of reduced signal. Fat repressed T2-WI and gadolinium amplified MR picture can be of use to show the cystic nature of dermoid cysts. Differential diagnosis is not very clear with epidermoid cyst and along with imaging, histopathological analysis is required to establish diagnosis.
It is best to remove the dermoid cysts surgically in patients who show symptoms.




{kind=link}