
INTRODUCTION:
Leptospirosis is a zoonotic disease that occurs worldwide, with an increased prevalence mostly in tropical and subtropical regions. The source of infection is generally direct or indirect contact with the urine of infected animals, such as rodents. Leptospirosis has become more common in urban areas owing to climatic change and poor sanitation. Leptospirosis is a common infection in rice-field workers due to prevalence of wild rats. Leptospirosis is known to cause various systemic manifestations, but in some rare cases, pancreatitis can occur. Thus, here is a case of acute pancreatitis associated with leptospirosis.
CASE REPORT:
This 68 years old gentleman with no known co-morbidities presented to us with complaints of fever for the past 4 days, for which he was prescribed paracetamol. In view of persistent fever he was admitted to outside hospital, on evaluation he had hypotension with elevated LFT, RFT, thrombocytopenia and leucopenia.
CT Abdomen :
Minimal peripancreatic fat strand with cholelithiasis.
Treated with antibiotics and Referred to our hospital for further management.
MANAGEMENT:
Initially managed as acute pancreatitis with MODS. CT Abdomen was repeated which showed Cholelithiasis. MRCP was done showed Cholelithiasis with no significant dilatation of intrahepatic biliary radicles. Tropical disease work up was sent to rule out other possibilities of MODS. Leptospirosis IgM came to be positive.
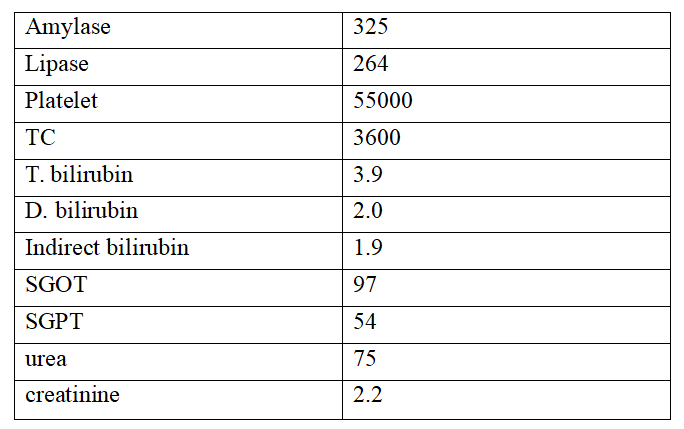
Lab investigations :
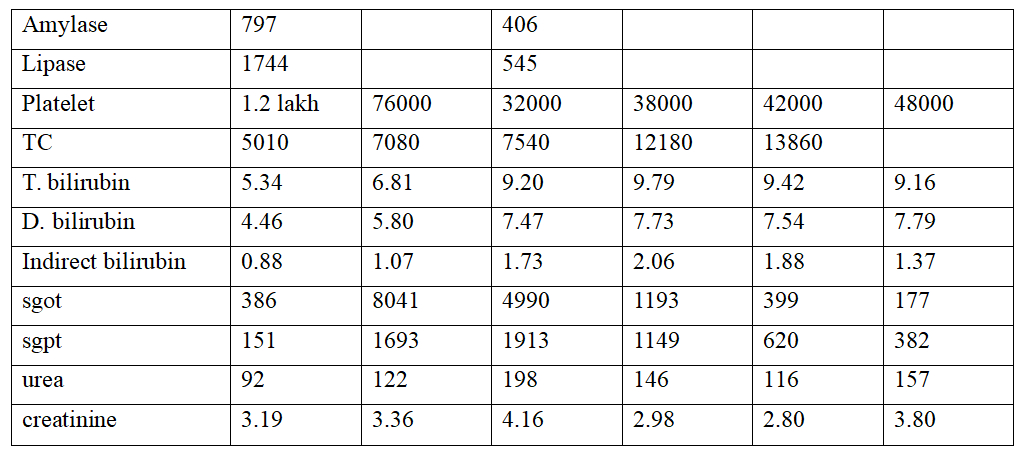
We continued with Inj. Meropenem and Doxy. In view of worsening RFT with oliguria he had undergone SLED. His lab parameters gradually improved except his RFT for which he required further sessions of HD and hence was discharged.
DISCUSSION:
Leptospirosis is a spirochetal infection. These bacteria infect humans by entering through the abraded skin, mucous membrane or conjunctivae. Direct transmission among human beings are rare.
Characteristic pathogenesis in development of Leptospirosis is vasculitis, endothelial damage, and inflammatory infiltration. The tissues mostly infected are the liver and kidney. In some cases pancreas may be affected and the primary pathology is due to vasculitis.
This disease presents as two spectrums: the most common (80-90%) anicteric leptospirosis and other one icteric leptospirosis. Icteric leptospirosis is known as Weil’s disease- is much more severe form than the anicteric spectrum, and it is characterized by hemorrhage, renal failure, and jaundice which is often rapidly progressing. Our case fits into icteric leptospirosis spectrum.
The acute renal failure in icteric leptospirosis can be either presented as oliguric or non-oliguric. It was observed in previous studies that oliguria was a significant predictor of death in leptospirosis. In our case it was oliguric presentation.
Jaundice occurring in leptospirosis is associated with hepatocellular necrosis which is also contributed by pancreatic and bile tree involvement and presents as impaired liver function. This is characterized by rise in transaminase levels which can be moderate – more than 2000U/dl, and there can also be minor elevation of alkaline phosphatase level. Hepatic dysfunction occurs but generally resolves, and it is usually a rare cause of death. The serum bilirubin level is usually less dhan 20 mg/dL but can increase upto 60-80 mg/dL. This increase in elevation of transaminases that is more than threefold of the normal value can occur.
For the diagnosing a case of acute pancreatitis, in a patient with abdominal pain there should be simultaneous determination of both amylase and lipase along with CT scan which is a gold standard. CT Abdomen has a 100% specificity and over 90% sensitivity for diagnosing acute pancreatitis. The presentations in acute pancreatitis can range from mild symptomatic illness to severe hemorrhagic pancreatitis causing peripancreatic necrotic collections and fatal multiorgan failure.
Diagnosis of leptospirosis in a patient who presents as acute pancreatitis is important because both acute pancreatitis and leptospirosis can lead to multi organ dysfunction, and early diagnosis along with appropriate management may reduce the risk of mortality.
The diagnosis of Leptospirosis is confirmed by either a positive PCR of blood or urine or by positive serologic testing; but rarely, diagnosis is made by a positive culture of blood or urine. The PCR tests has overall sensitivity of 40 – 60 % in blood, and the specificity is more than 95%. A single positive PCR is confirmatory of leptospirosis infection. However, the timing of collection of the sample in relation to the onset of symptoms determines the sensitivity of PCR. A negative PCR does not rule out leptospirosis since the leptospires presence in the fluids can be transient.
Serology test can be done by MAT, enzyme-linked immunosorbent assay (ELISA), immunofluorescence assay (IFA), lateral flow tests, and indirect hemagglutination tests and these measures specific immunoglobulin (Ig)M and IgG antibodies In case of culture by blood, urine, or CSF, the sensitivity of culture is suboptimal and Isolation of the organism is successful only in 5 to 50% of cases and also take several weeks.
TREATMENT
The treatment options for Mild disease in outpatient setting is with doxycycline or azithromycin.
In case of Severe disease, for those who are hospitalized – treatment with doxycycline (100 mg IV twice daily), ceftriaxone (1 to 2 g IV once daily), or cefotaxime (1 g IV every six hours) is usually recommended. The duration of treatment is usually seven days for severe disease.
CONCLUSION :
Leptospirosis should be considered as the differential diagnosis of elevated amylase with pancreatitis, and obstructive jaundice in endemic areas.
Acute pancreatitis is uncommon but may give rise to severe complications in patients with leptospirosis. To achieve a correct diagnosis in pancreatitis with leptospirosis a high degree of clinical suspicion and different modalities of investigations are essential. In patients with leptospirosis, acute pancreatitis can be missed because both conditions share similar clinical presentation and complications. When both Acute pancreatitis and leptospirosis are present there is high mortality and morbidity. Early diagnosis and appropriate treatment is essential for life saving.
REFERENCES :
- Leblebicioglu H, Sencan I, Sünbül M, Altintop L, Günaydin M. Weil’s disease: report of 12 cases. Scand J Infect Dis. 1996;28:637–639. doi: 10.3109/00365549609037976.
- Casella G, Scatena LF. Mild pancreatitis in leptospirosis infection. Am J Gastroenterol. 2000;95:1843–1844. doi: 10.1111/j.1572-0241.2000.02149.x.
- Edwards CN, Evarard CO. Hyperamylasemia and pancreatitis in leptospirosis. Am J Gastroenterol. 1991;86:1665–1668
- Kameya S, Hayakawa T, Kameya A, Watanabe T. Hyperamylasemia in patients at an intensive care unit. J Clin Gastroenterol. 1986;8:438–442. doi: 10.1097/00004836-198608000-00011.
- Moossa AR. Current concepts. Diagnostic tests and procedures in acute pancreatitis. N Engl J Med. 1984;311:639–643. doi: 10.1056/NEJM198409063111005.
- Desai A, Hattangadi D. Leptospirosis as a rare cause of acute pancreatitis. Internet J Surg 2008; 20.
- Prasanthie H, De Silva K. A rare complication of leptospirosis: acute pancreatitis. Galle Med J 2009; 13: 69.
- Daher Ede F, Brunetta DM, De Silva Júnior GBet al. Pancreatic involvement in fatal human leptospirosis: clinical and histopathological features. Rev Inst Med Trop Sao Paulo 2003; 45: 307–313.
- Schattner A, Dubin I, Glick Yet al. Acute painless pancreatitis as an unusual presentation of leptospirosis in a low-incidence country. BMJ Case Rep 2020; 13: e234988.
- P. Baburaj, T. Antony, F. Louis, B.L. Harikrishnan. Acute abdomen due to acute pancreatitis–a rare presentation of leptospirosis, J Assoc Phys India, 56 (2008), pp. 911-912.
pmc.ncbi.nlm.nih.gov/articles/PMC4434681
 Dr Ramapriya
Dr Ramapriya
Critical Care
Kauvery Hospital, Chennai
 Dr Vetriselvan P
Dr Vetriselvan P
Associate Consultant Critical Care Medicine
Kauvery Hospital, Chennai

{kind=link}