ABSTRACT:
Basilar thrombosis is a potentially fatal event, whose traumatic etiology has been repeatedly stated. Here we discuss about a case of 19 years girl who had basilar artery thrombosis secondary to road traffic accident
CASE PRESENTATION:
A 19 years aged girl presented to our Emergency department with alleged history of road traffic accident 4 wheeler vs 4 wheeler at around 2.30pm on 12/06/2022 near Dindivanam, she was immediately taken to Villupuram Government Hospital with GCS OF 15/15. Initially stabilized there and imaging done there included CT brain, CT whole spine and CT abdomen which were reported as normal study. She was hemodynamically stable with a GCS of 15/15 and was discharged.
At 2 pm on 13/06/2022 (the next day), she suddenly developed left upper and lower limb weakness for which she was initially shifted to nearby hospital, where she was evaluated and was found to be drowsy and disoriented. A Neurologist assessed the patient and had advised to shift to a higher centre for further management, hence she was shifted to our hospital for further management.
ON ARRIVAL IN ED:
Patient was afebrile, decreased response, not obeying commands
ON EXAMINATION:
- AIRWAY: threatened, not maintained with lots of secretions C- spine: Triple immobilization of cervical collar done
- BREATHING: RR: 22/min, SpO2: 98% at room air, Bilateral air entry present, no added sounds
- CIRCULATION: pt was having feeble peripheral pulses, HR – 98 /min, systolic BP: 90/60 mmHg, hypotensive
- DISABILITY: unconscious, not obeying to commands, minimal extension to painful stimuli, E3V2M3 (8/15), bilateral pupil equally reacting to light measuring 2mm, left UL & LL paucity of movements, CBG – 120 mg/dl
- EXPOSURE: Left side of neck & left axilla – seat belt marks +
INITIAL MANAGEMENT:
- Within 30 min of arrival in the emergency, patient developed right sided seizures with profound hypotension with a BP of80 mm Hg systolic, hence, in view of sudden drop in GCS, hemodynamic instability and threatened airway, after obtaining informed consent from the patient attender’s, patient was intubated with 8 size endotracheal tube & tube was fixed at 20 cm lip level after confirming position. Drugs used were IV thiopentone (induction agent) & IV rocuronium (paralytic agent).
- Post intubation her vitals were stable with a BP of 160/80mmHg, PR: 72/min, SpO2: 100% with Volume control mode.
- She was immediately shifted for repeat scans: CT brain showed hypo dense lesion 1.5 cm, multiple focal infarcts in the left superior cerebellar hemisphere, brain steam and right occipital lobe without mass effect
- CT whole spine done was normal.
- Her initial lab investigations showed – Normal counts, normal LFT, Normal RFT & electrolytes, hemoglobin: 13 gm%
- Her coagulation profile was also within normal limits
- ECG : normal sinus rhythm, ECHO showed trivial MR, no RWMA, normal LV function with EF: 60%
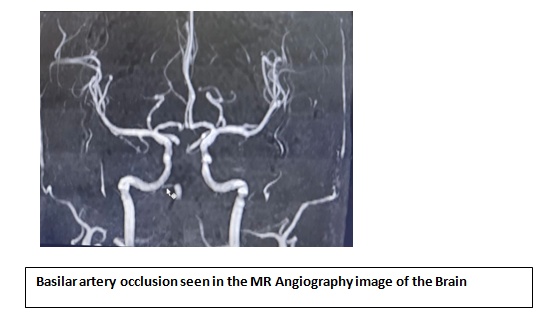
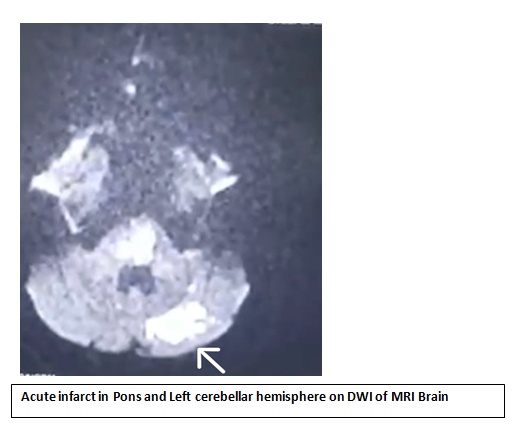
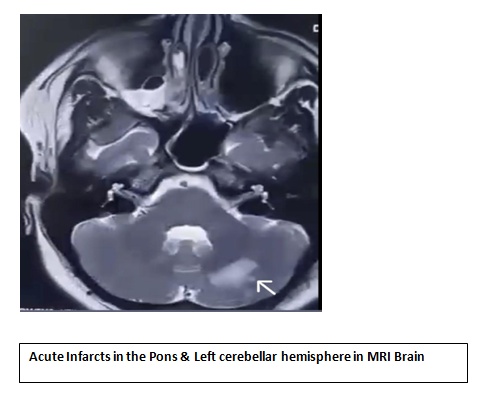
- She was shifted to ICU for further management and on further discussion with the neurologist on call, MRI brain with MRA was done showed abasilar artery occlusion with acute infarcts in the pons & left superior cerebellar hemisphere.
- In view of basilar artery thrombosis: after obtaining informed consent, patient was taken up for mechanical thrombectomy was done. The procedure was uneventful.
- She was then treated in the ICU and initiated on RT feeds and she underwent tracheostomy 5 days post admission.
- During her ICU stay, she developed coffee brown colour aspirate in the RT, for which endoscopy done showed gastric ulcer&hemoclipping was done.
- She was mobilized with the help of physiotherapist & a multidisciplicary approach for improving her overall condition was included in her care.
DISCUSSION:
- As in stroke, the common risk factor for basilar artery thrombus in 70% of cases is hypertension, coronary artery disease, cigarette smoking, atherothrombosis and hyperlipidemia.
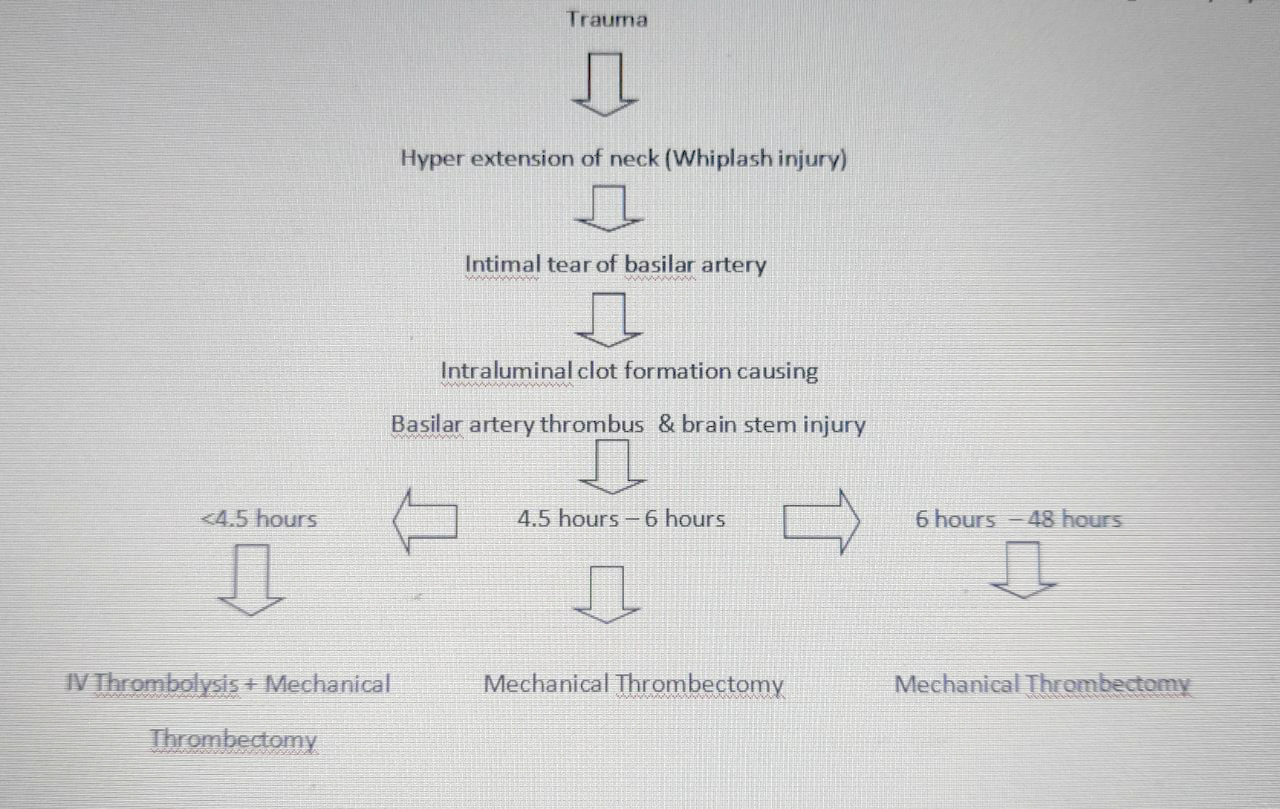
- A fatal basilar thrombosis can be related to minor trauma, soft tissue injuries of the cervical spine and its adjacent structure, especially when the mechanism of injury is more like a whiplash injury involving hyperextension of neck which is found to be a presdisposing factor towards vertebral artery thrombosis secondary to the tear in the vertebral artery. (1)
- In the above case scenario, patient had a road traffic accident and she was hemodynamically stable & conscious for 24 hours after which she developed left upper and lower limb weakness & low GCS.
- How did the RTA with whiplash injury of the neck caused the acute infarct and basilar artery thrombus, causing a delayed presentation?
- Trauma
- In this case, MRI showed a basilar artery thrombus and as it supplies the cerebellum, brainstem and occipital lobe, and these parts are responsible to control the level of conscious, coordination, balance and vision, patient developed low GCS at presentation.
- An intimal tear can occur with formation of an intraluminal clot, which may result in embolization in the posterior circulation. (2)
- In this case, if it was left untreated it may have lead to coma and death very quickly. But, as she was treated with mechanical thrombectomy, patient had a fairly decent outcome and now her present GCS is E3VTM3. (6T/15)
- She was normal for the first 24 hours, this has illustrated that an acute partial occlusion or a slow progressive occlusion with limited ischemic injury might have been there and, therefore, indicates a better prognosis if diagnosed early.
- Though IVThrombolysis & mechanical thrombectomy represents probably the best treatment that can be offered to victims of acute basilar artery occlusion (3) but from the above flow chart discussed, it is clear that early detection of the thrombus may have had better prognosis than the delayed detection, as time is crucial in initiating the IV thrombolysis.
- It is also clear that the patient had a very poor & guarded prognosis due to delayed presentation and she underwent mechanical thrombectomy, as it was the only treatment option in her case that which would probably reduce the overall mortality rate marginally.
- It is known that basilar artery thrombosis manifests in varied presentations including impaired consciousness, bulbar signs, weakness and sometimes even with vision disturbances, seizures and progresses to a semi-comatosed or comatosed state too.
- Despite the difficulties it poses to be picked up clinically due to its subtle presentations, it is still known to have a significant morbidity and mortality rate when diagnosed late but it has been found that with early detection and IV thrombolysis with mechanical thrombectomy the overall case fatality rate is reduced significantly. (1)
- Thus, we present a rare case of basilar artery thrombosis secondary to trauma, we wish to emphasize the need of early detection and treatment of basilar artery thrombus and have high index in trauma patient about brain stem stroke. (4)
- Hence, there should be a high index of suspicion of vascular injury in young person’s presenting with persistent unilateral head or neck pain even after a minor trauma should be maintained. This index of suspicion should be even higher in patients with posterior circulation symptoms with antecedent trauma
REFERENCE :
(1) Shaqiri E, Vyshka G, Sinamati A, Ymaj B, Ismaili Z. Fatal basilar thrombosis possibly related to minor cervical trauma: a case report. Case Rep Med. 2010;2010:401978. doi: 10.1155/2010/401978. Epub 2010 Aug 8. PMID: 20827380; PMCID: PMC2935134.
(2) Egnor MR, Page LK, David C. Vertebral artery aneurysm-a unique hazard of head banging by heavy metal rockers. Case report. Pediatr Neurosurg 1991-1992;17:135-8.
(3)Perttu J. Lindsberg and Heinrich P. Mattle Originally published26 Jan 2006https://doi.org/10.1161/01.STR.0000202582.29510.6bStroke. 2006;37:922–928
(4) Baird TA, Muir KW, Bone I. Basilar artery occlusion. Neurocritical Care. 2004; 3: 319–330. Crossref Google Scholar
 Dr. Mugundan. P.T
Dr. Mugundan. P.T
1st year Emergency Medicine Resident
Department of Emergency Medicine