Introduction
Stroke is the third leading cause of death in the western world. Only 50-60% of stroke survivors regain complete functional independence. The rest have varying degrees of disability. Hence it is very important to recognise the risk factors and prevent the stroke.
20% of strokes are haemorrhagic and 80% are ischemic. Causes of ischemic stroke are small vessel embolus originating from atherosclerotic plaque, cardiac source, prothrombotic conditions and other miscellaneous conditions. Carotid artery stenosis is one of the most common and correctible cause for ischemic stroke.
Case report
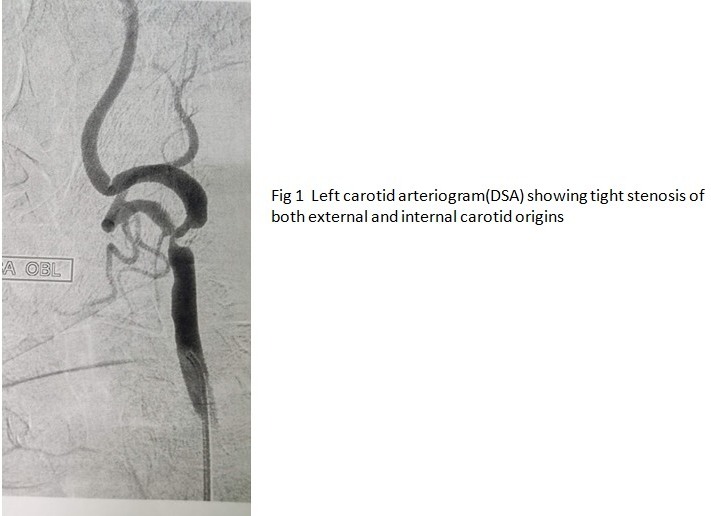
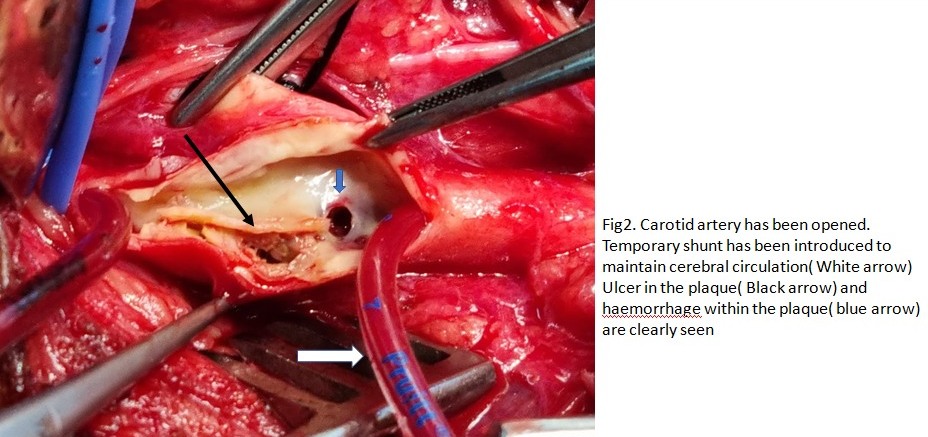
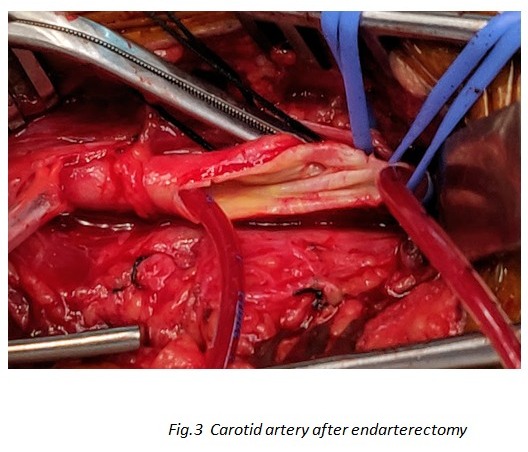
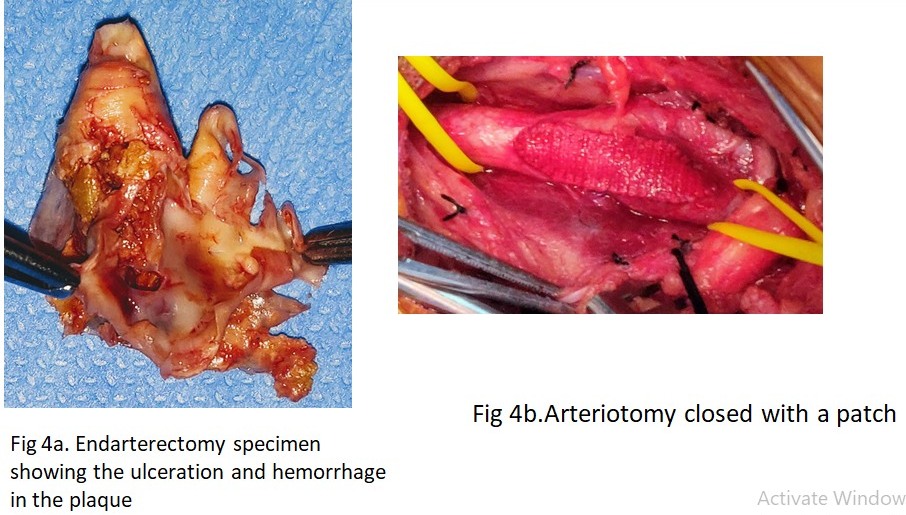
A 79-year-old hypertensive male with a past history of smoking presented with sudden onset right sided upper limb weakness, mental confusion and inability to communicate for four days. On examination he had right hand weakness, confusion, expressive dysphasia and right hemianopia. Right carotid thrill was present and bilateral carotid bruit was heard on auscultation. MRI brain showed acute infarct of left MCA and PCA territory (watershed area) He was treated conservatively with anticoagulation, antiplatelets, statins, anti-epileptic and antihypertensives. CT angiogram done showed bilateral calcified carotid arteries with 60-70%stenosis of right internal carotid artery (ICA) and 80-85% stenosis of the left ICA (Fig1). Carotid doppler showed raised peak systolic pressure in both internal carotid arteries confirming the presence of bilateral critical ICA stenosis. Cardiac evaluation was normal. Patient was taken up for left Carotid endarterectomy within two weeks of presentation. A temporary shunt was used to maintain the cerebral blood flow during the clam time. There was hemorrhage and plaque rupture (Fig2,) which was responsible for the embolization. Arteriotomy was closed after endarterectomy with a patch so that narrowing can be avoided (Fig 3, 4). Patient had an uneventful post op period and was discharged 4 days after the surgery on dual antiplatelets, statins, antihypertensive and antiepileptics. With regular physiotherapy hemiparesis has gradually recovered. At 30 days follow-up he was ambulant with good recovery of motor power and speech.
Discussion
Pathophysiology of carotid plaque
Carotid plaque usually occurs at the carotid bifurcation and causes narrowing of the origins of ECA and ICA. Infiltration of lipid into the arterial wall along with macrophage infiltration leads to gradual increase in the plaque size. Sudden increase in the plaque occluding the lumen can occur due to haemorrhage within the plaque. Alternatively rupture of the plaque can lead to discharge of debris which embolises causing TIA or stroke. Duplex scan can differentiate between this type of unstable plaque and a stable plaque.
Symptoms and Investigations
There are 3 types of clinical syndromes with symptomatic carotid disease. TIA or transient ischemic attack is defined as neurological events which last for less than 24 hours and full recovery occurs. Reversible ischemic neurological deficit(RIND) is when the neurological event lasts longer than 24 hours but resolves within 7 days. Stroke is defined as a focal loss of cerebral function with incomplete recovery.
Transient mono ocular blindness, dysarthria, dysphasia, aphasia, monoparesis, hemiparesis and hemisensory deficits are the common symptoms of TIA.
Duplex scan provides a useful screening and surveillance role in patients with carotid stenosis. It is fairly accurate in assessing the degree of stenosis and plaque morphology. The other imaging modalities are Magnetic resonance imaging and angiography, CT angiography and digital subtraction angiography. They are needed to plan intervention.
Treatment
Patients presenting with acute stroke within the golden hour(less than 3 hours after the onset) can be managed successfully by emergency thrombus aspiration and thrombolysis. Those who present later are managed medically first and investigated.
Based on the symptoms and degree of stenosis in the internal carotid artery, patients are planned for surgery or to continue best medical therapy.
Asymptomatic carotid stenosis is mostly treated medically. Best medical treatment includes strict abstinence from tobacco use, aspirin or clopidogrel or both, high dose statins, control of diabetes and hypertension, exercise and life style modifications.
Symptomatic extracranial carotid artery stenosis (50% to 99%) poses a high immediate and short-term risk of stroke. Without surgery, the 90-day stroke risk may be as high as 20% to 30%. Carotid endarterectomy has proven highly effective for reducing this risk
Carotid endarterectomy has been the most frequently performed open vascular surgical procedure for prevention of stroke. Several randomized prospective clinical trials have demonstrated the safety and efficacy of this procedure in the prevention of ischemic stroke in symptomatic patients with significant carotid stenosis.The incidence of perioperative stroke is about 1-3% which is much better than that after carotid stenting. The excellent perioperative results of this procedure reported in multicentre randomized clinical trials have made it the gold standard for carotid artery stenosis. A minimally invasive alternative is carotid artery stenting which carries a slightly higher risk of intra-operative stroke than carotid endarterectomy. Numerous studies have confirmed the long-term efficacy of carotid endarterectomy based in terms of stroke prevention as compared to carotid stenting. Carotid artery stenting is presently carried out for patients with contraindication to open surgical endarterectomy.
Timing of Surgery:
The timing of carotid endarterectomy for symptomatic carotid disease is a key benchmark for secondary stroke prevention because delays to endarterectomy are associated with an increased risk of recurrent stroke. The risk of recurrent stroke in those awaiting surgery was 12% at 4 weeks. A pooled analysis of the North American and European endarterectomy trials found that for patients with 50% to 99% carotid stenosis, surgery was most effective when performed within 2 weeks of the index ischemic event,
This time-dependent benefit was especially pronounced for patients with moderate (50% to 69%) carotid stenosis, in which endarterectomy was beneficial within the first 2 weeks, but the benefit was lost (and there was net harm) when surgery was delayed >3 months. The safety of performing carotid endarterectomy early has been demonstrated in several recent studies with perioperative morbidity and mortality rates comparable to that for delayed surgery in otherwise stable patients.
These data have changed practice guidelines for carotid endarterectomy. According to the American Academy of Neurology, “For patients with severe stenosis and a recent TIA or nondisabling stroke, carotid endarterectomy should be performed without delay, preferably within 2 weeks.”
Potential reasons for delays to carotid endarterectomy include patient factors (delayed symptom recognition and presentation to medical attention), physician factors (delayed diagnosis and referrals), resource availability (rapid access to vascular imaging), and institutional/system-level factors relating to operating room availability and staffing. Other potential reasons for delays to endarterectomy include a shortage of surgeons who perform this procedure and a lack of awareness about the timing of endarterectomy among family physicians and internists (who care for the majority of patients with stroke)
Summary
In patients with symptomatic ICA stenosis of >70%, Carotid endarterectomy (CEA) is shown to be beneficial in the first two weeks after an ipsilateral stroke or TIA. CEA is preferred over Carotid Artery Stenting(CAS) in older patients (>70 years). Studies have shown a higher procedural risk with CAS than CEA. Women have a less favourable benefit to risk ratio. Guidelines recommend intervention only if estimated perioperative mortality and morbidity risk is <6% for men and <4% for women. Guidelines recommend considering CEA in asymptomatic patients with over 70% ICA stenosis; if their perioperative risk is estimated to be less than 3%.
CAS may be considered for high-risk patients and those with anatomical contraindication for surgery. The benefit of carotid intervention for moderate symptomatic and asymptomatic ICA stenosis is unclear so far. There is no benefit in carotid endarterectomy if the carotid is 100% blocked
How to Prevent Stroke
Risk Factors
Risk factors important in stroke prevention can be divided into non-modifiable and modifiable risk factors.
Non-modifiable risk factors include
- Age (increased risk with increasing age)
- Race and ethnicity (higher risk of strokes in Africans than whites)
- Gender (higher risk for men, but this trend disappears beyond the mid-80s)
- Family history (especially of cerebral arterial disease)
- Genetic risk factors (for example, hypercoagulable states, sickle cell disease, cerebral amyloid angiopathy)
Modifiable risk factors
- Hypertension
- Diabetes mellitus
- Obesity
- Impaired lipid profile
- Atrial fibrillation
- Structural heart disease
- Carotid artery stenosis
- Lifestyle choices- Diet, Exercise, Smoking, Alcohol, etc.
In most cases, the patient has a combination of modifiable risk factors, i.e., hypertension, diabetes, high cholesterol.
Multiple risk factors increase the probability of stroke. Patients with identified risk factors can be educated in risk factors and decrease their risk.
Stroke prevention is the responsibility of all healthcare workers. Besides physicians, other health care workers can also help educate patients on how to reduce their risk of a stroke. Educating the patient on drug compliance with statins, anticoagulants, diabetic and antihypertensive medications. Smoking cessation and encouraging a healthy lifestyle also helps in reducing cardiovascular events.
Presenting Author: Dr. Rahul, MBBS, DNB (General Surgery)
Primary Author: Dr. N. Sekar, MS, MNAMS, MCh (Vascular), FICS, DSc (Hon. Causa), FRCS (Glasgow)
Past President – Vascular Society of India
Senior Consultant Vascular & Endovascular Surgeon
Dept of Vascular and Endovascular Surgery
Kauvery Hospital Chennai
Co-Authors:
Dr. S. Jithin Jagan, M.B.B.S., M.S.(General Surgery), M.R.C.S., M.Ch.(Vascular Surgery)
Dr. Archana, MBBS, DNB (General Surgery)
Dr. Dhilip, MBBS, MS (General Surgery)
 Dr. N. Sekar
Dr. N. Sekar Dr. Rahul
Dr. Rahul
{kind=link}