Scoliosis is a deformity of the spine resulting in lateral curvature and rotation of the vertebrae as well as deformity of the rib cage. Prior to surgical correction, a thorough pre operative assessment is essential as it involves preoperative multiorgan dysfunction, intraoperative blood loss and post operative pain management
CASE REPORT
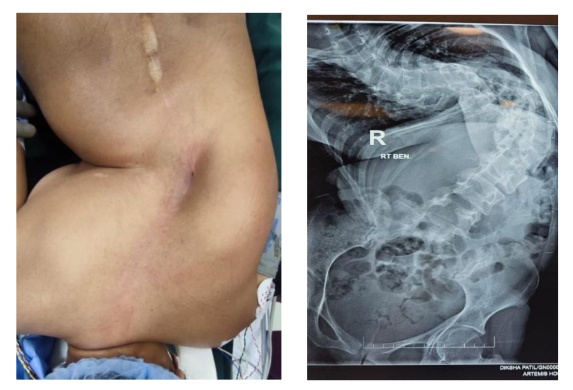
A 29-year female with history of neglected congenital scoliosis came for surgical correction. Clinical history showed no other congenital abnormality with poor cardiorespiratory effort. Cobb’s angle was found to be 150 degrees. PFT showed moderately severe restrictive pattern
No other neurological deficit was noted. Echo showed normal left ventricular function with no pulmonary artery hypertension
Pulmonologist and cardiologist opinion was sought preoperatively
PREOPERATIVE PLANNING
- A detailed discussion of the perioperative plan including intraoperative anaesthesia, need for massive blood transfusion and postoperative pain management clearly explained to the patient and the family
- Incentive spirometry was initiated and adequate blood products were reserved
ANAESTHESIA IMPLICATIONS
RESPIRATORY SYSTEM
- Pulmonary dysfunction can occur in spinal deformity.

- Pulmonary function testing (PFTs) will identify restrictive pulmonary deficits by showing decreased forced expiratory volume in one second (FEV1), decreased forced vital capacity (FVC) with a normal FEV1/FVC ratio and decreased Total lung capacity (TLC)
- Chest X-ray can be helpful in assessing the severity of disease. Cobb’s angle of ≥ 100 degrees is likely to cause severe cardiac and respiratory dysfunction
CARDIAC SYSTEM
- Chronic hypercarbia and hypoxemia due to pulmonary disease can lead to pulmonary hypertension and right ventricular failure
- Congenital scoliosis should be assessed for other associated cardiac problems such as cardiomyopathy, mitral valve prolapse, coarctation of aorta, mitral and aortic regurgitations
INTRAOPERATIVE MANAGEMENT
- Standard monitors including ECG, NIBP, pulse oximetry, temperature, and capnography was attached
- Bladder catheterisation was done for urine output monitoring
- Patient was induced with Inj Propofol 2mg/kg, Inj Fentanyl 2mcg/kg, Inj Cisatracurium 0.15mg/kg
- Right radial artery and Right IJV cannulation was done to aid in fluid administration
- Neuro monitoring was attached and patient was positioned in prone
- Proper padding of pressure points and eyes were done and double checked as it involves longer duration procedure
- Anaesthesia was maintained with TCI Inj Propofol and Inj Fentanyl
- Massive bleeding has occurred as expected during corrective surgery, which was promptly corrected with blood products.
- Blood samples were sent in the middle of the surgery as a part of massive blood transfusion protocol to check for PTINR, Platelet count and Serum fibrinogen levels which were found to be within normal limits
- Urine output was maintained at least 0.5ml/kg/hr
ANAESTHESIA IMPLICATIONS
HEMORRHAGE
- Scoliosis correction often requires a large incision with correction of multiple vertebral bones and can take longer duration. In prone positioning the vertebral veins become engorged from abdominal pressure and can contribute to increased blood loss
- Techniques such as continuous infusion of tranexamic acid, cell savage machines, prompt transfusion of blood products should be done
- Massive blood transfusion protocol should be used as deemed
- Goal directed fluid therapy should be employed for fluid correction
DURATION OF PROCEDURE
- It is definitely a long duration procedure
- Complications such as hypothermia, pressure point sores are expected
- Warmers, warm fluids should be used as hypothermia itself can cause coagulopathy and acidosis
- Eyes and pressure points should be adequately padded
- Cuff pressure should be checked at regular intervals
POST OPERATIVE CARE
- Surgery lasted for around 12 hours from induction, positioning, surgical time, repositioning to supine and weaning off from anaesthesia
- Patient was shifted to ICU for post operative elective ventilation and further management
- Patient was extubated the next day and iv fentanyl infusion was used for analgesia from the day of surgery
- Iv fentanyl infusion was continued for next 3 days
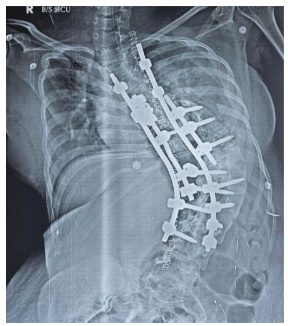
SECOND STAGE
- Patient was posted for second stage of scoliosis correction after four days
- It was also involved with major blood loss and longer duration
ANAESTHESIA IMPLICATIONS
- Postoperative pulmonary complications can occur in scoliosis correction and are more likely in more severe disease or syndromic patients
- PONV is very common post-surgery
- Postoperative pain management after scoliosis surgery can be challenging
- Multimodal approach to analgesia using paracetamol, NSAIDs, opioids and other available analgesics may improve outcomes. Patient-controlled analgesia has been reported to improve patient satisfaction
CONCLUSION
- A detailed pre-anaesthetic assessment and optimization of the respiratory and cardiovascular systems is very essential
- Important intraoperative considerations are vitals monitoring, temperature and fluid balance maintenance, positioning, spinal cord integrity monitoring and blood conservation
- With clinical experience of the Anaesthesiologist and expertise of the surgeon, kyphoscoliosis surgery can be made hassle free
 Dr. Mahalakshmi K
Dr. Mahalakshmi K Dr Nirmalraj Murugesan
Dr Nirmalraj Murugesan Dr. Hemalatha I
Dr. Hemalatha I Dr. Velmurugan Deisingh
Dr. Velmurugan Deisingh