A 45-year-old gentleman was brought to the emergency with a history of unconsciousness from the evening. On arrival, patient GCS was E4M5V2-11/15 and there was right hemiplegic. No known previous relevant history was noted
An emergency MRI brain with MRA of the neck and head was ordered and done.
MRI revealed large acute infarcts in the left MCA and bilateral ACA territory (Figure1)
Multiple acute lacunar infarcts were also noted in the left cerebellar hemisphere and bilateral frontoparietal and left occipital lobes.
However, no reformation of the bilateral anterior cerebral artery was seen. (figure2)
Occlusion of the mid and distal M 1 segment of the left MCA was noted (figure3)
A diagnosis of congenital agenesis of the bilateral ICA was considered, and CT brain was done for confirmation which showed absence of the bilateral carotid canals-(figure4)
Discussion
Agenesis of the bilateral ICA is a very rare congenital anomaly which is usually associated with other abnormalities like intracranial aneurysm and subarachnoid haemorrhage. Other structural brain anomalies are also possible, which can be associated with developmental delay.
ICA develops from the cranial prolongation of the distal third aortic arch and dorsal aorta during the third to fifth week, after which the skull base develops2so the development of the bilateral carotid canals essentially requires the normal formation of the bilateral ICA4
Mechanical or physical factors like amniotic band syndrome have been attributed to the congenital unilateral or bilateral carotid absence3
Essentially three types of collateral circulation come into play during unilateral or bilateral congenital agenesis i.e. from the opposite side ICA, persistentfoetal circulation, and the posterior circulation. In our patient, it was basically from the enlarged right PCOM artery. Unusual collateral circulation has also been described3i.e. primitive transmaxillary anastomosis originating from the right ECA.
The ophthalmic artery is the terminal branch of the ICA3. When the bilateral ICA is congenitally absent, the ophthalmic artery arises from the middle meningeal artery or the branches of the ACA.
In our patient, multiple branches were seen at the apex of the right orbit arising from the branches of the right external carotid artery.
In our patient, multiple branches were seen at the apex of the right orbit arising from the branches of the right external carotid artery (Figure5)
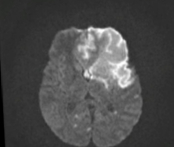
Figure 1 – Axial MRI brain showing acute infarcts of the left MCA and bilateral ACA

Figure 2 – Loss of Flow related signals of the bilateral intracranial ICA. There was a large calibre right PCOM perfusing both middle cerebral arteries
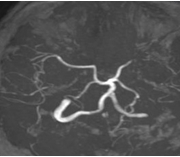
Figure 3 – MRA MIP images showing the bilateral MCA supplied by the posterior circulation
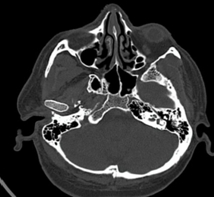
Figure 4 – Axial CT brain in bone windows showing agenesis of the bilateral carotid canals
Conclusion
Bilateral or unilateral ICA agenesis, although a critical finding, is usually an incidental diagnosis when evaluating for intracranial haemorrhage, TIA, or acute infarcts.
This is due to the fact that brain circulation is well established by collaterals from either one of the ways as described above. When the collateral is occluded or compromised by atherosclerosis, the patients become symptomatic.

Dr. Jeyabharathi Murali Kumar[1]
Radiologist
Kauvery Hospital