
Introduction:
Patients with chronic kidney disease are at increased risk for Cardio vascular morbidity and mortality. Various factors contribute to this risk including hypertension, anaemia, uraemia, mineral disorders, increased left ventricular hypertrophy and intra dialytic blood pressure fluctuations. (1)
Blood pressure changes are common during haemodialysis sessions (2). It could either increase, remain stable or decrease during a dialysis session. There are various factors that are responsible for these changes.
Fluid overload, increase in dialysate sodium, endothelial dysfunction, dialysability of anti-hypertensive medications, increase in sympathetic and RAAS activity. ESA usage, are some of the common causes of increase in post dialysis blood pressure.
Too much of ultrafiltration, myocardial stunning, ischemic heart disease, low dialysate sodium are common causes of low blood pressure post dialysis.
Greater the intra dialytic systolic blood pressure variability independently increases the cardio vascular mortality among dialysis patients. (3)
Aim: To study the intra dialytic changes in the systolic blood pressure in our maintenance haemodialysis patients.
Materials and methods: This is a retrospective, single centre study where all our maintenance dialysis patients systolic blood pressure pre and post dialysis were collected form our database. The last 6 haemodialysis sessions blood pressure recordings (pre and post) were noted and the average systolic blood pressures were calculated. This is to avoid the bias of depending on single recordings of blood pressure in defining their blood pressure variability.
Based on the blood pressure variability patients were categorized into 3 groups. Those in whom the blood pressure “increased” post dialysis by >5 mm Hg (Group A), in whom the blood pressure remained “stable” post dialysis (between +5 and – 5 mm Hg- group B) and those in whom the blood pressure “decreased”> 5 mm Hg (group C)
Patients baseline clinical characters including age, gender details, the basic renal disease were compared with the blood pressure changes.
Statistical analysis was performed using SPSS, (Version 23.0). The continuous variable will be expressed as Mean and Standard deviation. Categorical variables will be expressed as frequency and percentage. Independent ‘t’-test will be used to find the significance difference between groups. Correlations relationship between two variable analysed by applying Pearson’s coefficient. Chi- square test and fisher’s exact test will be used to find out association between the categorical variables. P < 0.05 will be considered as statistically significant.
Results: Total number of patients were 175 (Mean Age 57.58 + 15.2 years) Male: Female 121: 54 Diabetic nephropathy was the basic disease in 90 and 85 patients had non diabetic ESRD.
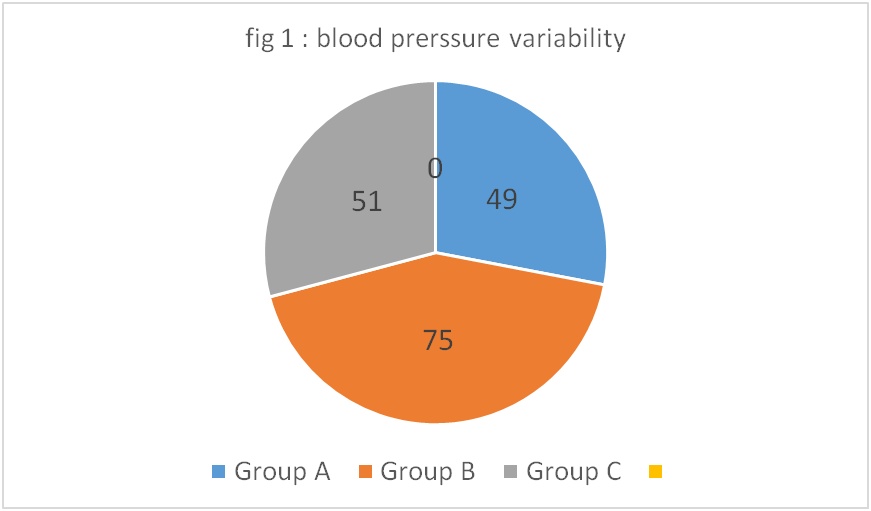
49 patients had increase in post dialysis blood pressure of > 5 mmHg (group A), stable blood pressure in 75 patients(group B) and decrease in blood pressure beyond 5 mmHg was seen in 51 patients (group C). The mean age in these groups were 56.37 +16.49, 58.87 + 13.71 and 56.84 + 16.15 respectively.
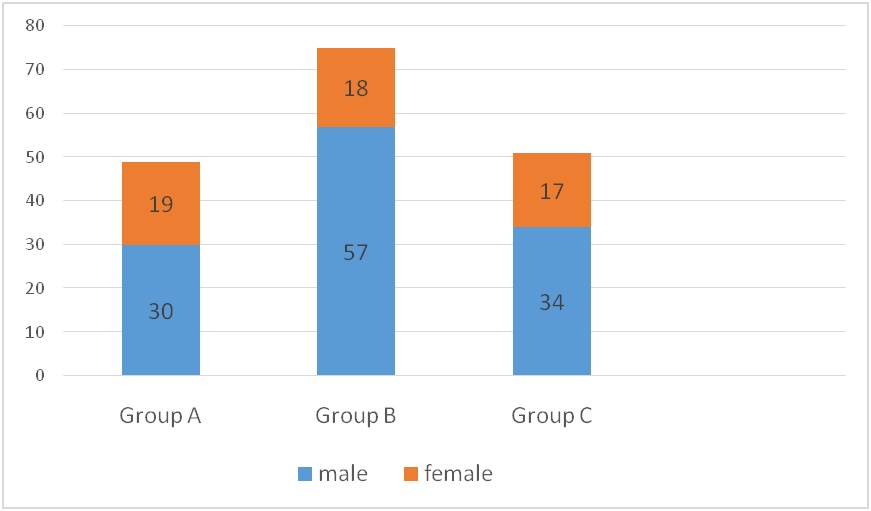
The gender distribution among these group are as follows. In Group A gender ratio was 30:19, in Group B it was 57:18 and in Group C it was 34 :17 (x2 = 0.198 NS)
Fig 1 – Gender distribution in BP groups
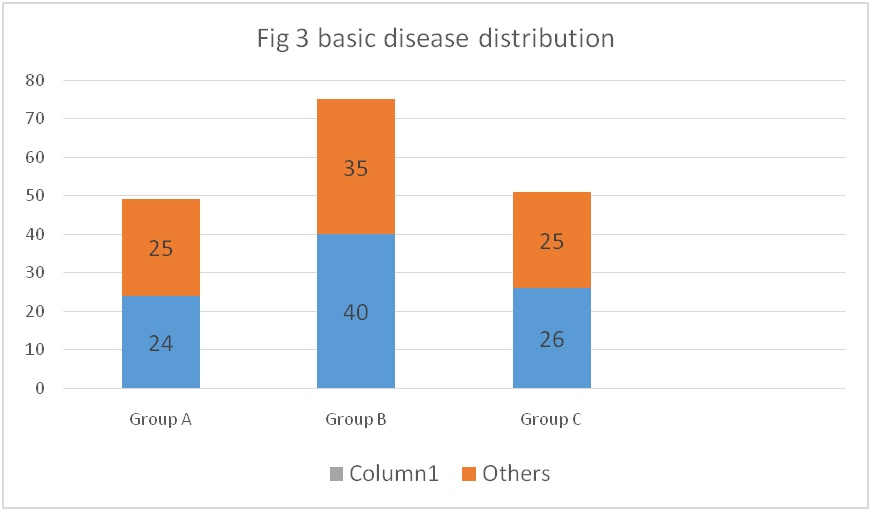
There were 90 patients with Diabetic nephropathy and 85 patients had non diabetic renal diseases. ( x2 = 0.891 NS)
Among them the distribution of blood pressure variability in Group A 24:25, in Group B 40: 35 and in Group C 26: 25
References:
- Burton JO, Jefferies HJ, Selby NM, McIntyre CW. Hemodialysis-induced cardiac injury: determinants and associated outcomes. Clin J Am SocNephrol. 2009 May;4(5):914–20
- Levin NW. Intradialytic hypertension: I. Semin Dial. 1993;6:370–371
- Anika T Singh et al, Association of different definitions of Intradialytic hypertension with long term mortality in Dialysis patients 2022;79:855–862 ( PROVEN that any increase is associated with increased mortality)
- Jennifer E.Flythe ,Jula K . Inrig , Tariq Shafi. Intradialytic Blood Pressure Variability Is Associated With Increased All-Cause and Cardiovascular Mortality in Patients Treated With Long-term Hemodialysis. Am J Kid Dis 2013Jun: 61(6) : 966-74




{kind=link}