INTRODUCTION:
Hypercalcemia is a relatively common manifestation in clinical practice. It results when the entry of calcium into the circulation exceeds the excretion through the urine or deposition into the bone. The common causes are primary hyperparathyroidism, malignancy, hypervitaminosis D. Here we report a case with severe hypercalcemia and associated with sarcoidosis.
CASE REPORT:
A 55 yrs. old female with history of long standing type 2 Diabetes mellitus and SHTN, normal renal function test 6 months before, presented with complaints of significant weight loss around 20kg over past 6 months, nausea and constipation. Initial blood workup revealed deranged renal function (creatinine – 4.36mg/dl) and malignant hypercalcemia (serum ca – 16.69mg/dl) other tests with in normal limits. Hypercalcemia was treated with IV fluids, steroids, diuretics and calcitonin nasal spray intact PTH and Vitamin D levels were with in normal limits. CT Chest showed multiple enlarged mediastinal lymph nodes. Serum ACE levels were elevated-93.9U/L(normal range 12-68). To rule out malignancy ,serum protein electrophoresis showed no para protein peak. AFP, CEA, CA 19-9 were all negative.
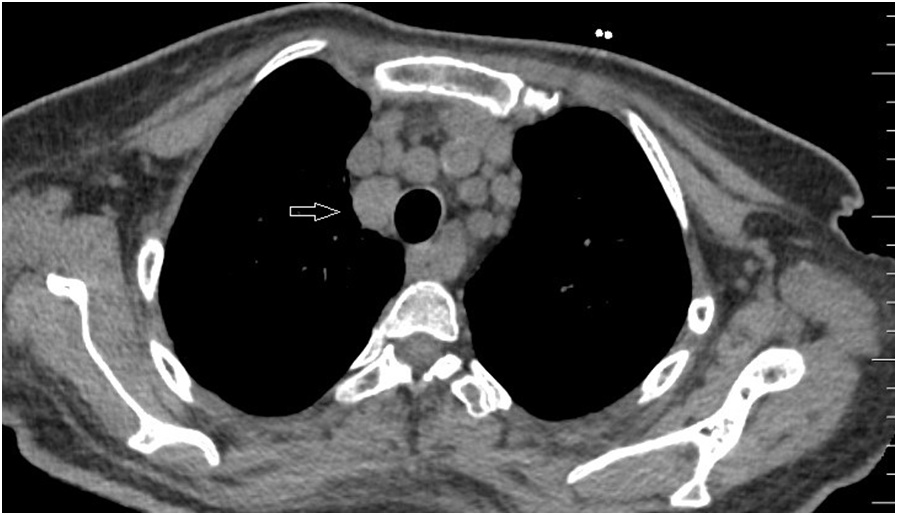
Figure1: CT chest showing mediastinal lymphadenopathy
PET scan revealed multiple mediastinal bilateral hilar, left axillary and periportal and upper retroperitoneal fluoro deoxy glucose (FDG) nodes with mild metabolic activity. To rule out lymphoma, through EBUS, FNAC of the lymph nodes done showed Necrotising granulomatous inflammation, negative for malignant cells. Gene-Xpert for tuberculosis was negative. Sarcoidosis was confirmed with above investigations and started on Prednisolone 30mg OD. Patient improved symptomatically. Currently she is on tapering dose of steroids. Serum creatinine improved to 1.6mg/dl.
DISCUSSION:
Sarcoidosis is a multisystem granulomatous disorder of unknown etiology that affects individual worldwide and is characterized pathologically by the presence of non caseating granulomas in involved organs.
Serum ACE level is elevated in 75 percent of untreated patients with sarcoidosis. However it has limited utility as a diagnostic due to poor sensitivity and in sufficient specificity.
Moderate elevations in serum calcium concentration(12-15 mg/dl) can cause reversible decline in glomerular filtration rate that is mediated by direct renal vasoconstriction and natriuresis induced volume depletion.
Longstanding hypercalcemia and hypercalciuria may lead to degeneration and necrosis of the tubular cells and eventual tubular atrophy and interstial fibrosis and calcification(nephrocalcinosis).
Steroid therapy is the first line management for hypercalcemia associated with sarcoidosis because it reduces the calcium level through the inhibition of osteoclast function and decreases calcium absorption from the gastrointestinal tract.
REFERENCES:
- Baughman RP, Teirstein AS, Judson MA et al.. Clinical characteristics of patients in a case control study of sarcoidosis. Am J RespirCrit Care Med2001;164:1885–9. 10.1164/ajrccm.164.10.2104046 [PubMed] [CrossRef] [Google Scholar]
- Adams JS, Singer FR, Gacad MA et al.. Isolation and structural identification of 1,25-dihydroxyvitamin D3 produced by cultured alveolar macrophages in sarcoidosis. J ClinEndocrinolMetab1985;60:960–6. 10.1210/jcem-60-5-960 [PubMed] [CrossRef] [Google Scholar]
- Krikorian A, Shah S, Wasman J. Parathyroid hormone-related protein: an unusual mechanism for hypercalcemia in sarcoidosis. EndocrPract2011;17:e84–6. 10.4158/EP11060.CR [PubMed] [CrossRef] [Google Scholar]
- A. R. Berliner, M. Haas, and M. J. Choi, “Sarcoidosis: the nephrologist’s perspective,” American Journal of Kidney Diseases, vol. 48, no. 5, pp. 856–870, 2006
- Rudruidee Karnchanasorn,1Molly Sarikonda,2Saleh Aldasouqi,3and Ved V. Gossain Severe Hypercalcemia and Acute Renal Failure: An Unusual Presentation of Sarcoidosis
 Dr.S.Vishnu Shankar
Dr.S.Vishnu Shankar
First Year DrNB (Nephro)
Resident
Department of Nephrology

{kind=link}