INTRODUCTION
A variety of anaesthetic techniques are available for patients undergoing vascular surgical procedures. General anesthesia used for most of the carotid, aortic, and peripheral artery bypass surgery. Neuroaxial blockades can also be used in lower extremity revascularisation if there are no contraindications. Regional nerve block is considered as great alternative in high risk patients. Nerve block can be used for various reasons including post op analgesia, surgical procedure and chronic pain syndromes
CASE REPORT
A 58 years old female, ASA IV, weighting 38 kg with history of RHD with severe mitral stenosis S/P MVR in 2014. Now came with complaints of left leg pain and intermittent claudication. Patient was also diagnosed with Acute on chronic kidney disease on that admission and nephrologist opinion obtained before the surgery.
The patient and her family were informed about the surgical and anaesthetic procedure and possible complications. The informed consent form was signed. On physical examination, weight 38 kg, blood pressure 100/40 mmHg, heart rate 118 bpm; lucid, oriented, and collaborative; cardiac auscultation with irregular rhythm, low pitch murmur in the apex region; respiratory auscultation revealed breath sounds with bilateral basalcrepts, mallampati 2, limited neck mobility. Pre-op ECG AF with controlled ventricular rate, Echo- Normal functioning mitral prosthesis in position with normal mitral valve gradient, severe LV systolic dysfunction, severe pulmonary artery hypertension (PAH-63 mm hg), No clots, RV dysfunction also present, EF 20-25. Hb 10.7, platelet 264000, INR 1.3, creatinine 1.4, Urea 77. Patient has functional capacity of less than 2 mets. Denies any allergic history.
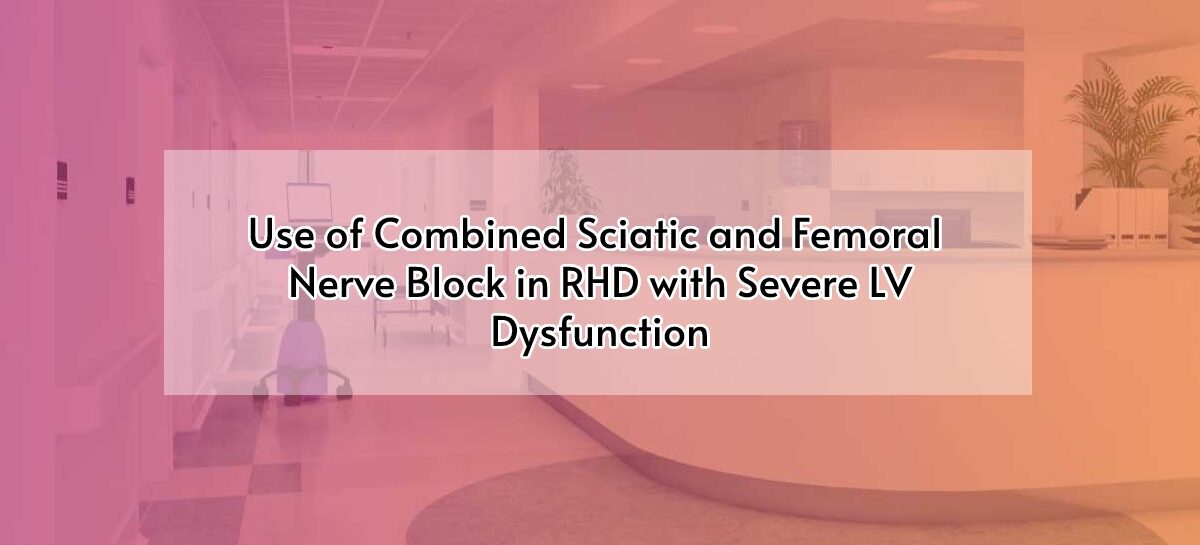
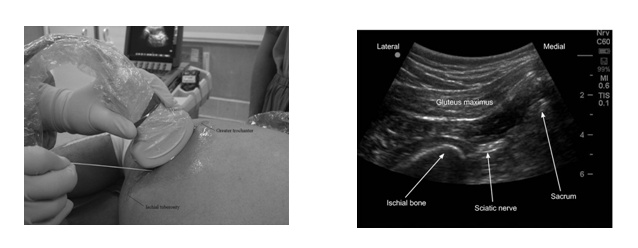
In the operating room patient was positioned in supine position. ECG, SpO2, radial artery cannulated for IBP. Patient was sedated with midazolam 1mg and fentanyl 50 mcgs. Combination of ultrasound guided femoral and sciatic nerve block were performed. Sciatic nerve was performed using subgluteal technique with aid of ultrasound and nerve stimulator. Nerve block solution was prepared using 15 ml of 0.5% ropin, 15 ml of 2% lox with adrenaline, 4 mg of dexamethasone, 5 ml of distilled water. During the procedure, heparin 5000 units was administered before clamping the femoral artery. The procedure lasted three hours without complications. In the postoperative visit the next day, the patient presented with minimal pain in the left lower limb (3/10 on numerical scale) and without motor blockade.
DISCUSSION
Chronic arterial occlusion is a disease most often caused by atherosclerosis. Patients are usually asymptomatic because of compensatory collateral circulation; however the main symptom intermittent claudication appears when there is damage to blood vessels.
The goal of anaesthesia in this patient is to maintain hemodynamic changes without any further deterioration of pre-existing condition. Doing the procedure under general anaesthesia is a concern in this patient because as there will be hemodynamic instability due to severe LV dysfunction and low ejection fraction. Neuroaxial blockade is contraindicated in this patient due to possibility of bleed and hematoma formation at the site of injection as the patient was on LMWH, anti-platelets and anticoagulants and patient also has severe LV dysfunction.
The best alternative for this patient is nerve block where we can achieve same amount of analgesia and anaesthesia as in neuroaxial blockade. We can either combine sciatic and femoral nerve block or sciatic and lumbar plexus block together. But in this patient we chose sciatic and femoral together to avoid sympathetic blockade which can lead to hypotension in lumbar plexus block as said above to have minimum hemodynamic variations.
Regional block is also effective in blocking the surgical stress response and also provides post-operative analgesia. However, it is difficult to perform in obese and uncooperative patient and in long duration procedures.
SCIATIC NERVE BLOCK
Sciatic nerve block is a good technique for lower limb anesthesia and analgesia. When combined with femoral nerve block, it provides knee, leg, and foot analgesia and with posterior lumbar plexus block it provides femur, thigh, knee, leg, and foot analgesia. The sciatic nerve is formed by the union of the lumbosacral trunk L4-L5 and anterior branches of the S1-S3 roots. It emerges from the pelvis through the sacrum sciatic foramen, passes below the piriformis muscle in a deep plane in the gluteal region, then goes down the midline of the back of the thigh, and divide itself in the popliteal fossa in tibial nerve and fibular nerve.
FEMORAL NERVE BLOCK
The femoral is an easy procedure to be performed under ultrasound guidance. Femoral nerve is formed by L2-L4 roots, in thigh itsposterior to the inguinal ligament and passes laterally to the femoral vessels. It is found deeper and lateral to the femoral artery. The fascia lata, which passes over the nerve and the vessel, and iliac fascia that passes over the nerve, but below the femoral vessels. Femoral nerve block provides analgesia in the anterior side of the thigh skin, most of the hip joint, knee joint, quadriceps muscle, and skin of the medial side of the leg and foot.

CONCLUSION
Nerve block can be considered as one of the best alternatives in patients with high risks in whom GA or neuroaxial blockade can cause further deterioration in pre-existing condition.
REFRENCE
- Anaeesthesia for lower extremity vascular bypass with peripheral nerve block Jordana de Fraga Guimarãesa,Cristine Formighieri Angoneseb,c, Rafael Klein Gomesb, Vasco Miranda Juniora,b, Carlos Fariasb,d.
- Use of Femoral and Sciatic Nerve Block Combination in Severe Emphysematous Lung Disease for Femoral Popliteal Arterial Bypass Surgery Onur Selvi, OlgarBayserke, SerkanTulgar



{kind=link}