Percutaneous Coronary Intervention (PCI) or Coronary Angioplasty has evolved in leaps and bounds ever since Andreas Gruentzig’s first successful coronary angioplasty treatment on an awake human performed on 16 September 1977 where he expanded the narrowed lumen of the coronary artery with use of balloon. PCI is now an effective solution in many patients with atherosclerotic Coronary Artery Disease (CAD) presenting as ANGINA or ACUTE MYOCARDIAL INFRACTION. From the initial days of Plain balloon angioplasty that lead to risks of acute vessel recoil and acute closure following PCI and restenosis in intermediate to long term follow up research in this field started offering more and more solutions by way of Bare metal stent that addressed the immediate acute vessel closure enhancing the procedural success of PCI, leaving re-stenosis unaffected. Drug Eluting Stents – DES platforms were introduced and significant advances in the drug, its polymer coating and the drug delivery with designs in stent struts found an effective way to minimise the re-stenosis to less than 3%. Thereafter PCI was consistently applied as an alternative mode of coronary revascularisation to many complex lesion subsets like Bifurcation, Chronic total occlusion, long and diffuse disease and left main as well. Currently PCI is offering complimentary revascularisation solutions to subjects who are otherwise candidates for Surgical revascularisation through Coronary Artery Bypass Graft (CABG).
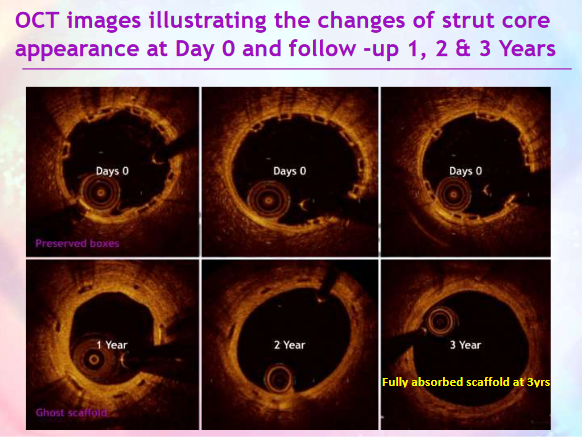
Notwithstanding the above significant advances in PCI techniques and technology along with similar stride in Dual Anti-Platelet agent use, there were cases of late / very late stent thrombosis due to variable endothelial coverage of the stent struts with its late mortality in those who received DES. There were also many patients who were young and DES platforms left permanent metal material within the coronary arteries. This led to research into evolution of Bio-Resorbable Scaffold – made of Poly-Lactyl-Lactic-Acid polymer-based scaffolds that became available for human use and is completely resorbed by scavenging mechanisms in human body system over a period of 30 to 36months leaving the vessel segment to be back to normal near natural state except for the metal markers at the ends of these scaffolds.
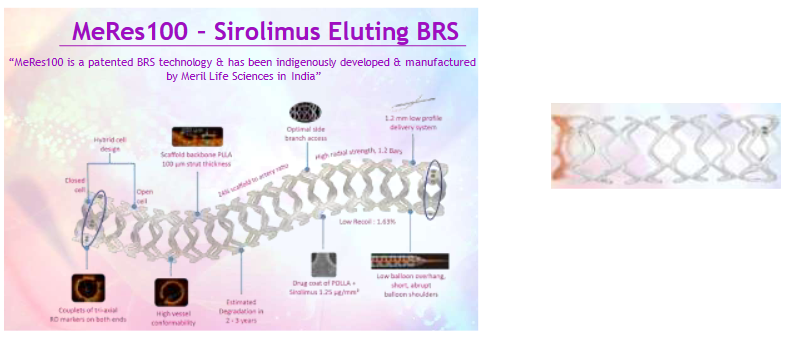
The first generation of this bio-resorbable scaffold – ABSORB –was approved and introduced in 2012 and soon endorsed by the interventional cardiologist world-wide. However, there was a rise in scaffold thrombotic risk that exceeded that from use of DES. This scaffold thickness lead to partial endothelial coverage as well. The ABSORB scaffold was then withdrawn globally but did not cease the interest in the further technical modification of the Bio-resorbable scaffold. The currently approved MeRES 100 – is a novel 100micron thick bio-resorbable PLLA scaffold has been tested and found safe and effective among Indian CAD patients. MeRES 100 has been available for human use for PCI since January 2021 and currently its use is restrictive for few types of CAD lesions that are short segment involvement in vessels over diameter 2.75mm or more up to 4.0mm. As CAD affects many young subjects in India, this MeRES Bio-resorbable scaffold offers an effective PCI solution to many with single or multi-vessel CAD involvement and retains the option of further PCI or CABG surgery should the atherosclerosis disease progresses in these patient subjects in future unlike metal jacketed DES in the vessels that precludes graft anastomosis in such vessels implanted with DES.
Further there are many CAD patients in India with diffuse atherosclerotic vessel involvement as well as having small calibre vessel diameter of <2.50mm which is not uncommon. Recent advances of drug delivery into the vessel wall by nano-technology spheres coated with Sirolimus directly without stents or scaffold has made great strides in treating this diffuse and small calibre vessel CAD involvement. Sirolimus Drug Coated / Eluting Balloon (sDEB) technology now therefore gives significant options to revascularize vessels that were neither amenable for bypass grafting nor stent implantation. The combination of the new technologies of Bio-Resorbable 100MICRON SCAFFOLD and Sirolimus Eluting Balloon has now made a reality of METAL-LESS PCI solutions – an emerging horizon for select patients with multi-vessel / single vessel CAD involvement among our population.
MeRES Bio-Resorbable Scaffold:
At Kauvery Hospital Chennai in the past 1 year, the author has had successful experience of using the above 2 technologies in treating 30 patients with CAD through the META-LESS PCI. All the 30patients has had 100% procedural success rate with no in-hospital or 30days major adverse cardiac events(MACE). The mean follow up has been 6months with range of 30days to 14months. There was no scaffold thrombosis with current generation of DAPT use and no deaths among the 30 patients cohort. Of these patients, 1 patient had multi-vessel Metal-less PCI with Sirolimus Drug Eluting balloon alone without scaffold use. The following are the illustrated cases of the Metal-less PCI concept of newer PCI solutions that has emerged currently.
METAL-LESS PCI CASE 1:
35 years gentleman heavy cigarette smoker, with hyperlipidemia presented with Unstable Angina of Class III, normal LVEF and Stress test evidence of significant ischemia. His coronary angiography showed single vessel Proximal Left Anterior Descending (LAD) artery critical >90% focal discrete tandem stenosis.
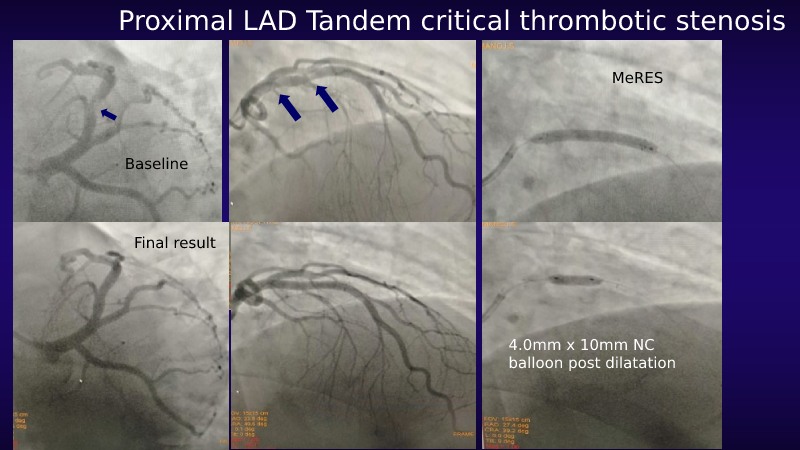
This patient was successfully treated with implant of the 3.50mm x 29mm MeRES BIO-RESORBABLE Scaffold. There were no procedural complications and no recurrence of angina in the past 12months. He is followed up with DAPT, High dose statins and BP lowering medications till date. He has been rehabilitated to quit smoking completely.
METAL-LESS PCI CASE 2:
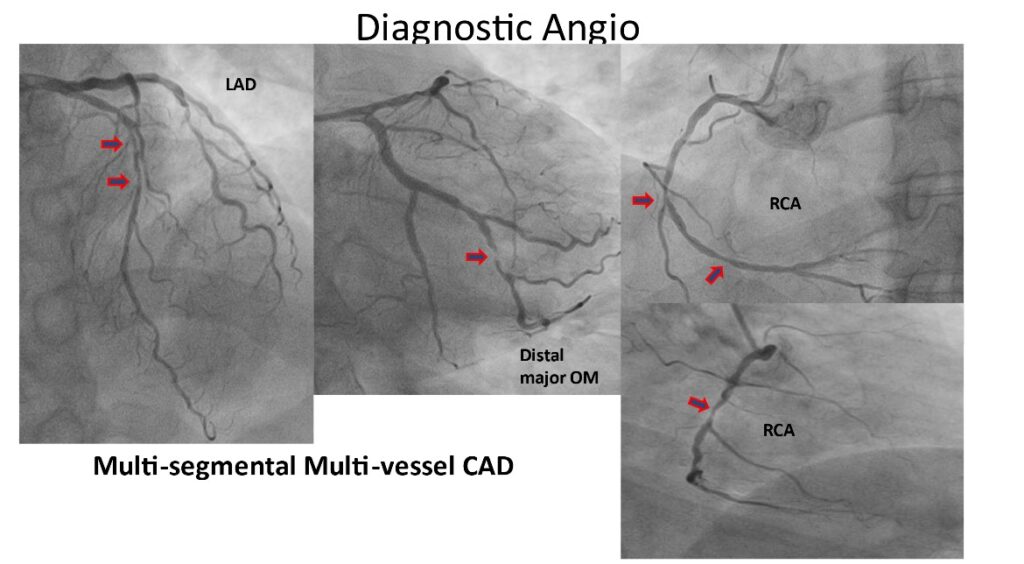
53 years gentleman with Type 2 Diabetes mellitus, Systemic Hypertension, Strong family h/o premature CAD, Hyperlipidemia – refused to take statin after his first ACS event in 2012 when he had single vessel Diagonal vessel involvement for which medical management was recommended. This gentleman presented 4months ago with progressive Class II angina during activities of daily living and had poorly controlled glycemic state of HbA1C >8%, and LDL-C 186mg/dL. His coronary angiography showed multi-vessel critical CAD involving proximal to mid LAD, major Obtuse marginal (OM) vessel and multiple segments of right coronary artery (RCA).
He was advised CABG surgery being a diabetic and multi-vessel CAD involvement. However, patient did not consent for the CABG surgery and preferred to undergo multi-vesselPCI without metallic DES implants.
Therefore, this middle-aged gentleman had successful staged – 2 stage – multi-vessel PCI with multiple MeRES Bio-Resorbable scaffold implant and use of 2 sirolimus drug eluting balloon use for the PCI. He recovered well with no 30day MACE and is angina free for past 120days while continuing DAPT, High dose statin, OHA with basal Insulin doses.
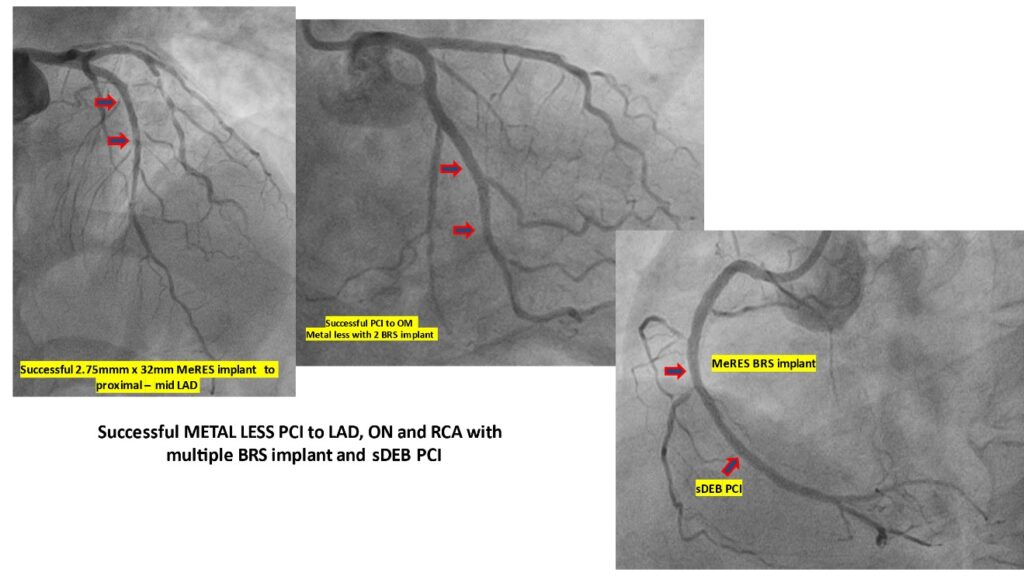
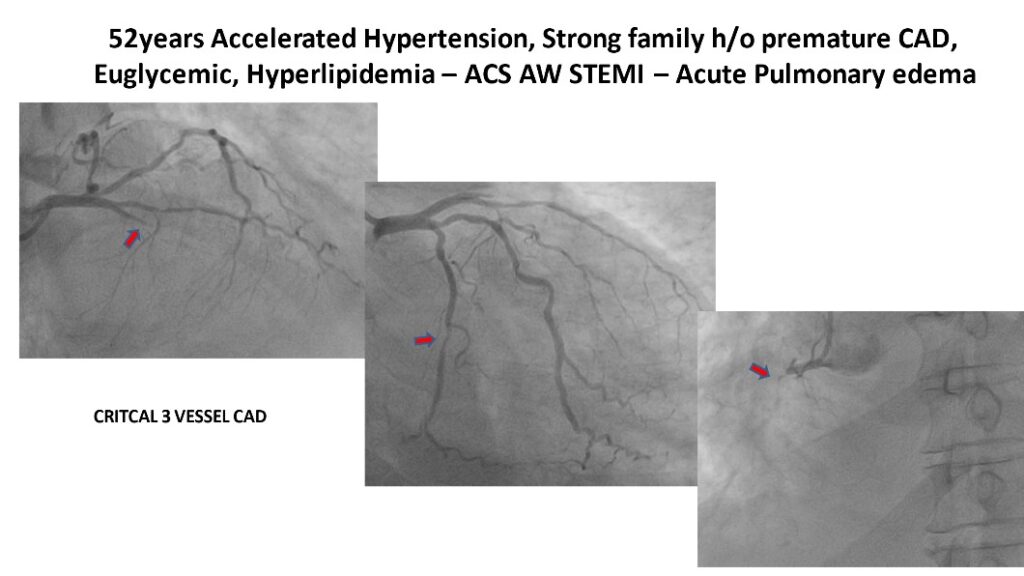
METAL-LESS PCI CASE 3:
52years well-built gentleman with Type 2 Diabetes mellitus, strong family h/o premature CAD, Systemic Hypertension, Hyperlipidemia on medical follow up presented with abdominal bloating, dyspepsia and shortness of breath initially seen by medical GE specialist and without relief. Presented to ER with Class IV breathlessness to ER and noted to have Acute Anterior Wall STEMI complicated by acute pulmonary edema and severe LV dysfunction. He was immediately taken up for emergency coronary angiography that showed mid LAD 100% occlusion, a major diagonal >70% tandem stenosis, mid Circumflex (Cx) artery discrete ~70% stenosis and critical near total occlusion of proximal RCA.
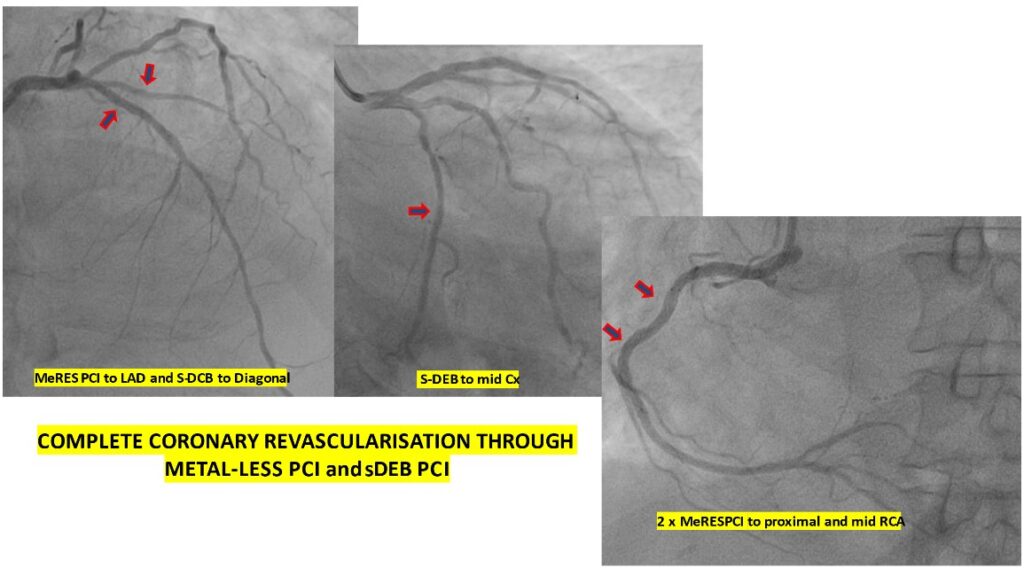
Due to STEMI presentation with heart failure, successful primary PCI with Bio-resorbable MeRES scaffold was implanted to LAD vessel. He improved from heart failure in 3 days’ time in CCU and then had successful multi-vessel staged PCI with sirolimus Drug eluting balloon PCI to diagonal and mid Cx segments followed by 2 Bio-resorbable MeRES scaffold implant to proximal and mid RCA. This gentleman had staged multi-vessel complete Coronary artery revascularisation through metal less technology with a combination of DCB and Bio-resorbable scaffold. At 30days follow up this patient is in NYHA Class II and LVEF ~38%.
METAL LESS PCI CASE 4:
COMPLETE REVASCULARISATION FOR 3 VESSEL CAD ONLY THROUGH s-DEB TECHNOLOGY
WITHOUT SCAFFOLD AND ONLY DCB TECHNOLOGY – truly metal-less and scaffold-less PCI
48years lady with Systemic Hypertension, Hyperlipidemia presented elsewhere with chest pain of 3 days and diagnosed as NSTEMI ACS and then came to this facility. Her LVEF WAS ~48%. Her coronary angiogram showed small calibre <2.50mm 3 vessel critical CAD involving proximal LAD that showed >90% stenosis with 2 OM disease and normal RCA. As the vessels were small in calibre and feasibility of grafting through CABG surgery was questionable, this lady had successful multi-vessel PCI to LAD, LCx and RCA by use of Sirolimus Drug Eluting Balloon PCI alone without DES or Bio-resorbable scaffold implant.
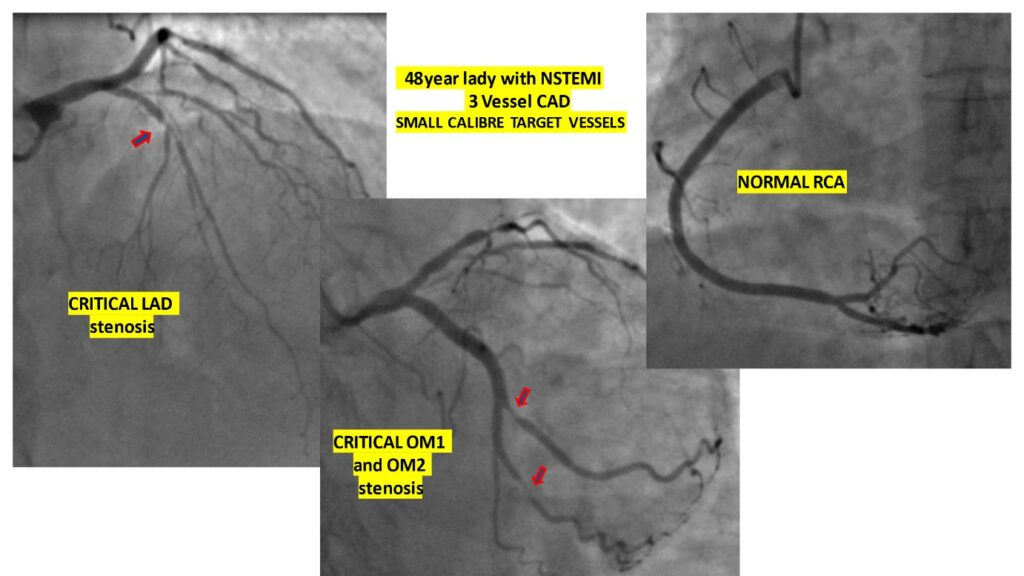
At 45days follow up she is asymptomatic in NYHA Class II and LVEF ~55%.

The scaffold and sDEB PCI solutions mandate meticulous vessel bed preparation of the lesion with appropriate balloon pre-dilatation followed by intra-coronary imaging through IVUS / OCTfollowed by right size Scaffold implant or sDEB use without causing any vessel injury or dissection at the target site and a final post dilatation using the appropriate size balloon for scaffold optimisation. All these steps performed in a seamless manner leads to greater success of the PCI in the selected patient with CAD. Procedural success of Bio-resorbable scaffold PCI is at par with PCI using DES.
These cases illustrate the current evolving horizon of METAL LESS PCI to many of our young or not so young patients with CAD regardless of their multi-vessel disease involvement. Currently both the MeRES BIO-RESORBABLE Scaffold technology and the Sirolimus Drug Eluting Technology – MAGIC TOUCH – balloon are MAKE IN INDIA advanced PCI solutions and offers a disruptive evolving comprehensive PCI treatment for our patient populations with small calibre coronary vessel involvement and multi-vessel CAD. The objective of not to leave anything permanently in the coronary artery vessels is achieved with success and keeps the scope for future coronary revascularisation choices open for these patient subjects.
These cases portray a disruptive approach to current practises of PCI in DES era. All experiences in medical science have evolved with First in Man successful use of the therapy followed by more selected patient population that are closely followed up as in our experience.
At Kauvery Hospital Chennai, the author has maximum experience of use of Drug Eluting balloon PCI and Bio-resorbable scaffold PCI in this part of India.
 Dr. Manoj Sivaramakrishnan
Dr. Manoj Sivaramakrishnan
Senior Consultant & Interventional Cardiologist
Kauvery Hospital Chennai