
Case History: Mrs. L, 75 years old female known to have Diabetes and Ischemic heart disease was admitted with severe congestive cardiac failure. She needed stiff doses of IV diuretics, CPAP, inotropic support and other cardio protective measures. She was hemodynamic stable and her renal functions were normal. She remained breathless, needing CPAP and her urine output remained less than 1000 ml per day for 4 days.
Her ECG did not reveal any acute coronary event, ECHO revealed diastolic dysfunction, USG revealed dilated cardiac chambers, tricuspid and gross mitral regurgitation and congestive hepatomegaly.
Nephrologist opinion was asked for, and she underwent “Isolated Ultra filtration” and she recovered subsequent to 17 liters of fluid removal over 4 days,
Discussion:
1. What is diuretic resistance?
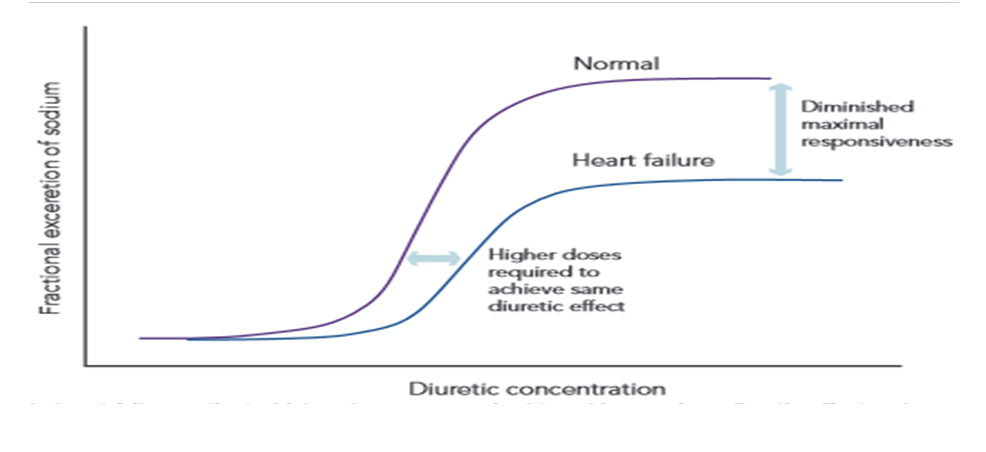
Persistent fluid overload in spite of adequate diuretic dose and failure to obtain a therapeutic result in edema reduction. Urinary sodium of <90 mmol/l is considered as diuretic resistance. In cardiac failure increased diuretic dose is needed compared to normal individuals to get a diuretic response (1)
2. What are the reasons for diuretic resistance?
Extra renal reasons – reduced renal blood flow, renal venous congestion, ascites, increased dietary salt intake, hypoalbuminemia
Renal causes – decreased GFR, decreased diuretic delivery to the tubules, diuretic braking phenomenon, increased distal sodium delivery, metabolic alkalosis etc.
3. What is Compensatory post diuretic sodium reabsorption?
The diuretic is expected to increase the sodium loss. But after the loop diuretic phase, if the urinary sodium is < 20 mmol/l it is defined as compensatory sodium reabsorption. Fortunately it is not that significant in volume overloaded CCF patients.
4. What is the alternative approach if there is diuretic resistance?
Isolated Ultra filtration is considered as a viable alternative to iv diuretic therapy. Enough studies are available that compared the diuretics to ultra filtration. Most of the studies confirm the beneficial effects of ultra filtration. Reduction of volume is significant in ultra filtration compared to diuretic therapy (2).
5. What are the advantages of ultra filtration?
Predictable fluid removal, isotonic ultra filtration hence much more sodium removal compared to diuretic therapy, no neurohumoral activation, no hypokalemia, better diuretic response post therapy
6. What are the disadvantages of ultra-filtration?
Need for vascular access, anti coagulation need, bleeding risks, catheter associated infection are some of the concerns.
References:
⦁ European cardiology review. Diuretic therapy in heart failure – current approaches. 2015 :10 (1) 42-47
⦁ Maria Rosa Costanzo JACC Heart Fail 2016 Feb;4(2):95-105.
 Dr.R.Balasubramaniyam, MBBS, DNB( Gen.Med), DNB(Neph)
Dr.R.Balasubramaniyam, MBBS, DNB( Gen.Med), DNB(Neph)
Head, Department Of Nephrology
Kauvery Hospital, Chennai

){kind=link}