A 45-year-old female (height 165 cm; weight 141 kg; body mass index 51 kg/m2) was scheduled to undergo robot-assisted surgical staging for endometrial cancer. She is a known case of T2DM, SHTN, Hypothyroid, Asthmatic and OSA on CPAP for 10 years.
PRE-OPERATIVE PLANNING
- Routine investigations were done and pulmonologist opinion was sought in the view of OSA/ Asthma prior to surgery.
- Blood investigations found to be within normal limits, Echo revealed Normal LV function, No PAH
- Polysomnography showed severe OSA whereas PFT doesn’t show major abnormality.
- Patient was asked to admit a day before the surgery. She was asked to continue routine medications till day of surgery. A dose of LMWH was given 12 hrs prior to surgery for DVT prophylaxis
- Plan of anaesthesia and risks associated with anaesthesia in this case scenario were clearly explained to the patient and attenders’
- Nebulisation and pre medications – Inj Pantaprazole 40mg iv, Inj Palanosteron 0.075mg were given
- Suitable Table which can withstand a patient weight of up to 250 kg regardless of position was arranged
INTRA OPERATIVE MANAGEMENT
- The patient was positioned supine and all monitors were attached – pulse oximetry, non-invasive blood pressure (NIBP) and electrocardiogram (ECG).
- Ramped position was used during induction and preoxygenated with 100% O2 via facemask

- She was anaesthetized with propofol 200 mg IV and suxamethonium 100 mg IV, Fentanyl 100mcg iv and successfully intubated with 8mm ID endotracheal tube in first attempt with assistance of laryngoscope
- Arterial line and central line were secured and anaesthesia was maintained with TCI propofol infusion at 3mcg/ml effect site concentration
- Inhalational agents and further dose of opioids were avoided to prevent post operative excessive drowsiness
- Adequate paddings were kept to prevent pressure injuries
- The patient was placed in a steep Trendelenburg lithotomy position (30° head down), and pneumoperitoneum was created with CO2 insufflation at a pressure of approximately 15 mmHg
- Mechanical ventilation was performed by pressure control ventilation with Fi02 40% and the respiratory rate was adjusted to maintain end-tidal CO2 at between 35 and 45 mmHg.
- Analgesics such as Inj Paracetamol 1g, Inj Diclofenac 75mg and adequate local infiltration of local anaesthetics over incisional site were used
- Surgery was completed without any hemodynamic instability and shifted to ICU with maintenance iv sedation
POST OPERATIVE MONITORING
- The patient was reversed with Neostigmine and Glycopyrrolate and extubated after regular respiration with good tidal volume
- After successful extubation, the patient was kept in non-invasive ventilation and then changed to the regular BiPAP
- Post operative analgesics such as Inj Paracetamol, Inj Tramadol were suggested
- Inj Enoxaparin was used for DVT prophylaxis
- She was successfully ambulated on POD 2 without any significant post operative complications
CASE DISCUSSION
Obese surgical patients pose multiple challenges to the anaesthetist.
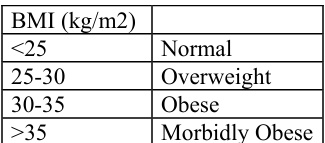
Obesity is associated with other medical co-morbidities such as diabetes, hypertension, cardiopulmonary disease, venous thromboembolism, and psychosocial disease.
AIRWAY AND RESPIRATORY SYSTEM
- Obese patients are at increased risk of having difficult airways, as bag mask valve ventilation and intubation can be challenging.
- Better predictors of difficult intubation
- Greater neck circumference (>42 cm)
- Higher Mallampati score (>3)
- BMI >50 kg/m2
- the presence of a beard
- One of the frequent complications associated with obesity is obstructive sleep apnoea (OSA).
- A high index of suspicion of OSA are symptoms such as witnessed snoring, excessive somnolence during the day, choking and coughing bouts at night, awakening from sleep multiple times during the night.
- Pulmonary and systemic vasoconstriction, polycythaemia, right ventricular failure and cor pulmonale can occur
Anaesthesia Implications
- Careful history should be taken for the symptoms of OSA
- Avoid sedative premedication.
- Maintenance of the airway might be difficult. Airway obstruction is very likely to occur in the postoperative period
CARDIOVASCULAR SYSTEM
- Obesity is a significant coronary heart disease risk factor.
- These patients should undergo a thorough cardiovascular examination prior to surgery.
- Investigations should include chest X-ray, 12-lead electrocardiography and polysomnography in patients with OSA
Anaesthesia Implications
- Blood pressure arm cuffs should be long enough to encircle at least 75% of the arm and 40% of the width of the arm
- Obese abdomen will directly compress venous return from the legs increasing the risk of deep vein thrombosis DVT
- DVT prophylaxis, TED stockings and early mobilisation are some measures to reduce the incidence of DVT.
VENTILATION
- Obese patients have increased oxygen consumption and CO2 production because of increased total body tissue mass
- This can lead to hypercapnia and hypoxaemia when ventilation is impaired. Excess adipose tissue reduces chest wall compliance, which reduces functional residual capacity (FRC)
Anaesthesia Implications
- These patients are prone to hypoxia
- Due to the reduced chest compliance, higher pressures are required to ventilate patients
- Extubation is usually best performed with the patient in the sitting position as awake as possible to allow maximal diaphragmatic excursion.
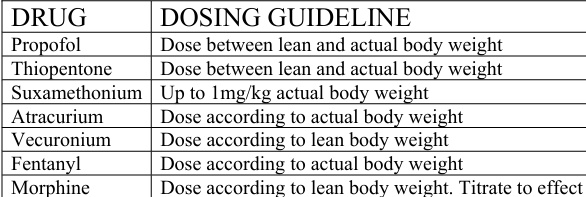
DRUG HANDLING
In the obese patient, volumes of distribution, binding and elimination of drugs are unpredictable
CONCLUSION
Morbidly obese patients require meticulous approach in both pre operative assessment and post operative management. Anaesthesia should be tailored to the physiological changes seen in obesity and the presence of comorbidities.
 Dr Hemalatha
Dr Hemalatha
Department of Anaesthesia
Kauvery Hospital, Chennai
 Dr Nirmalraj M
Dr Nirmalraj M
DNB Resident 2nd Year
Department Of Anaesthesia
Kauvery Hospital, Chennai