High risk patients for anesthesia refers to patient comorbidities which will definitely have anesthesia related hemodynamic changes irrespective of the surgery or procedure. In these patient’s nerve blocks give the best outcome for anesthesia and analgesia.
Who comes under the high-risk category?
⦁ Morbidly obese
⦁ Geriatric patients
⦁ Ischemic heart disease, poor lv contractility, high pulmonary artery pressure
⦁ Chronic kidney disease
⦁ Peripheral vascular disease
⦁ Lung disease/ poor lung reserve
Anesthetic agents have a direct impact on sympathetic & parasympathetic autonomic nervous systems causing myocardial depression resulting in hemodynamic instability. Whereas in the nerve block there is no such harm we will be witnessing. In high risk patients we avoid additives in nerve block as they may cause change in heart rate, blood pressure, respiratory depression, delirium and dementia for example dexmedetomidine and long acting opioids. By this we even reduce the post-operative nausea, vomiting, sore throat which is commonly seen after general anesthesia.
Most commonly nerve blocks are administered for procedural anesthesia and analgesia in the following procedures:
⦁ Limb procedures
⦁ Orthopedic surgeries
⦁ AV graft
⦁ Plastic surgeries
⦁ CAPD catheter insertion
⦁ Hernia repair
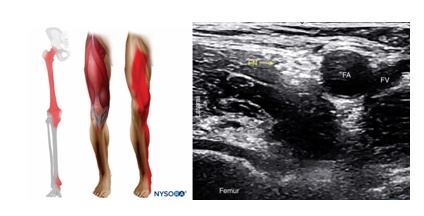
Upper limb nerve blocks give us the choice to focus on the localized site of surgery. The brachial plexus blocks from proximal to distal in anatomical order of the brachial plexus: interscalene, supraclavicular, infraclavicular, and axillary. Lower limb blocks are femoral nerve, sciatic nerve, popliteal nerve, ankle block which covers the foot. Abdominal blocks are rectus sheath, transabdominal plane block, ilioinguinal nerve and field block for hernia repair.

Drugs commonly used for nerve blocks are 0.25% bupivacaine, 2% lox with adrenaline, 0.5% and 0.75% ropivacaine calculated according to the site of block and duration of surgeries
Nerve blocks are contraindicated in patient query of nerve injury and infection at the site of infection.
Case Report 1:
60yr old male patient came for emergency with obstructed inguinal hernia, he is a known case of diabetic, ESRD-CKD (2018) on medical management with creatinine of 7.4,obstructive uropathy. RECENT ACS NSTEMI on 26/8, echo showed significant rwma+, moderate Lv dysfunction, ABG showed compensated metabolic acidosis. After explaining high risk for anesthesia pt was taken up under TAP + FIELD BLOCK with sedation.
In our clinical practice being a geriatric center, patients with multiple comorbids, it’s quite challenging to optimize them completely as their physiology & pathology which is not going to change. In these patients’ nerve blocks become the life saver for patients and anesthesiologists.
Case Report 2:
71yr old male patient chronic diabetic& hypertensive, coronary artery disease with EF25%, CKD on medical management presented with acute lower limb ischemia. Taken up for right popliteal tibia bypass surgery. Pt was taken under femoral + sciatic nerve block
DISCUSSION
Our main anesthetic GOALS is to maintain normotension, heart rate +/- 20 beats from the baseline, oxygenation, volume replacement, and post-operative pain relief. In these high risk patients, nerve blocks are the best choice of anesthesia. There is hardly any change in hemodynamics, hypotension is avoided. Hence no change in cardiac and renal blood flow. Also no need to load fluid to maintain volume status as there is no hypotension. The patients need not be kept nil oral post-surgery. The patients can be started on oral intake once they are back to the recovery room. Which in return avoids hypoglycemia, dehydration side effects. These patients are in chronic pain, we are usually left out with less choice of analgesics due to their age, reduced renal reserve, and long term use of NSAIDS makes them resistant to analgesics.
Nerve block helps in prolonged duration of action and adequate immediate post-op pain relief for 12-18hours.
CONCLUSION
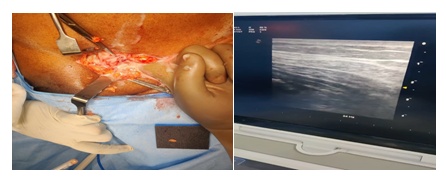
Patients with complicated systemic illness, nerve blocks have least pharmacologic trespass to the patient, no sympathetic & parasympathetic disturbance. Nerve block is considered the safest choice of anesthesia with ultrasound practice which gives us the visualization of nearby vascular structures, also the drug deposition which helps us not to exceed the dosage, early recovery and adequate analgesia.
Speedy recovery is no longer a wish, It is a Fact.
 Dr. Mahalaksmi . K ,
Dr. Mahalaksmi . K ,
Consultant Anesthesiologist
Kauvery Hospital Chennai