
INTRODUCTION:
While dealing phobic patient conscious sedation plays an important role in alleviating fear, anxiety and pain. It is a safe method which reduces the need for general anesthesia especially in day care dental procedures.
WHAT IS SEDATION?
Sedation is the reduction of irritability/ agitation by administration of drugs generally to facilitate a patient for diagnostic, interventional, medical or surgical procedure for the process of producing a degree of impaired response with or without loss of consciousness.
WHAT IS CONSCIOUS SEDATION?
Conscious sedation is a technique in which the use of a drug or drugs produces a state of depression of the central nervous system (CNS) enabling treatment to be carried out, but during which verbal contact with the patient is maintained throughout the period of sedation. Conscious sedation retains the patient’s ability to maintain a patent airway independently and continuously.
In conscious sedation the patient can responds to verbal commands or light tactile stimulation. Patent airway and spontaneous ventilation can be maintained in conscious sedation. Conscious sedation does not impair independent respiration and normal cardiovascular function. The principal hazard of moderate sedation is induction of excessive sedation with a deeper than desired level of anesthesia and the potential for hypoventilation and hypoxia.
DEPTH OF SEDATION
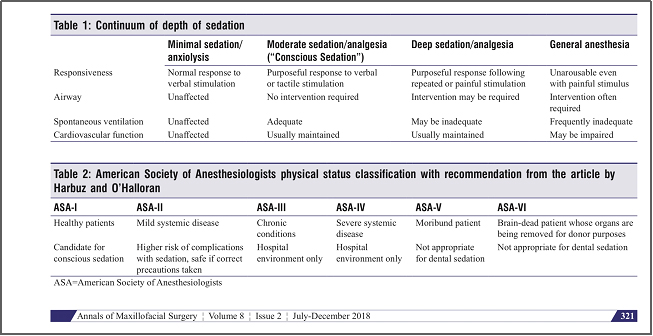
PATIENT SELECTION FOR CONSCIOUS SEDATION
Patients under category ASA 1 and ASA 2 are considered for dental procedures in peripheral settings and ASA 3,4 should be done under hospital setting. Patient should be throughly evaluated prior to the procedure including detailed history, airway, fasting, ASA status of the patient should be established. Before the start of the procedure one must ensure about the availability if airway equipments, venous access and appropriate intraoperative monitors are available.
CHALLENGES FACED DURING CONSCIOUS SEDATION IN DENTAL CHAIR
- Availability of manpower and monitors
- 2.Shared airway between the dentist and the anaesthesiologist.
- Anxiety and phobia.
- Respiratory obstruction might be possible in children with enlarged tonsils and adenoids.
- Cardiac arrhythmia due to nerve stimulation
- Risk of patient losing consciousness, respiratory and cardiovascular depression
- Vasovagal syncope.
HOW TO OVER COME IT?
- Through examination of the patient prior to the procedure.
- The same standards of personnel, monitoring and equipment should apply whether anaesthesia is administered in a hospital or in a dental surgery.
INDICATIONS :
- Phobia and anxiety
- Traumatic and long dental procedures
- Medical conditions aggravated by stress such as angina, asthma and epilepsy
- Children
- Mentally challenged individuals
- Ineffective local anesthesia due to any reason.
CONTRAINDICATIONS OF CONSCIOUS SEDATION
- Obese patient, OSA
- Congenital Heart Disease associated with CHF or cyanosis, COPD
- Patient with Raised Intracranial Pressure and neurological impairment.
- Uncooperative and unwilling patient.
- Lack of equipment or inadequate personnel of the patients as an individual.
METHODS AND DRUGS COMMONLY USED FOR DENTAL SEDATION
- Before administration of drugs either by inhalational routes or by intravenous route it is mandatory to secure I.V line in patient
INHALATIONAL AGENTS: Sedation with inhalational agents is extremely useful in children and in patient with needle phobias.
NITROUS OXIDE: Nitrous oxide can be used alone with proxygenating the patient and then titrating the concentration from 30% and increasing it according to desired level of sedation. Entonox mixture (50% oxygen and 50% nitrous oxide) can also be used.
SEVOFLURANE: Sevoflurane can be used as a sole agent mixed with air or oxygen to cause conscious sedation or it can be combined with nitrous oxide to produce the same. A MAC of 0.3 to 0.5 produces significant sedation.
PARENTERAL AGENTS (IV OR IM):
OPIODS – Fentanyl or Remifentanyl are short acting opiods which can be used in conscious sedations. Usually opiods are used in combination with other agents.
BENZODIAZEPINES : Benzodiazepines has wide margin of safety. Diazepam and Midazolam effective for conscious sedation and most commonly used. These drug has sedative, anxiolytic properties and can produce amnesia.
KETAMINE : Trance-like state of sensory isolation provides a unique combination of amnesia, sedation, and analgesia while preserving vital brain stem functions. Ketamine at titrated dose can preserve cardiovascular and respiratory functions despite producing profound amnesia and analgesia.
PROPOFOL: When used in lower doses, it induces conscious sedation. It has a short half-life and thus the recovery from sedation is much faster than for midazolam. In addition, propofol has no active metabolites and undergoes prompt hepatic clearance after intravenous administration.
DEXMEDITOMEDINE – Dexmedetomidine is a relatively new drug, which can cause sedation. It has sedative, anxiolytic properties and analgesic Dexmedetomidine induces dose-dependent effects, ranging from minimal to deep sedation.
ORAL OR TRANSMUCOSAL AGENTS:
Benzodiazepines are most commonly used oral agents. To achieve it desired effect it should be given atleast 1 hour prior. Other agents like zaleplon can also be used.
Fentanyl can be administered by parenteral, transdermal, nasal, and oral routes. Fentanyl lozenges available in a variety of strengths, from 200 to 1600 µg. Onset of action with in 5 to 10 minutes. Fentanyl lollipops of dose 20 to 50 mcg produces desired analgesic and desired effect. It is most accepted route in children.
MAD – MAD (MUCOSAL ATOMIZATION DEVICE)- this device causes Atomization of drug produced fine particles (30-100 micron in diameter). Drugs are sprayed intranasally which causes less discomfort during administration and increase drug absorption. Due to its non invasiveness it can be easily used in children.
WHAT ELSE CAN BE USED IN SHARED AIRWAY PROCEDURE?
THRIVE – Transnasal Humidified Rapid Insufflation Ventillatory Exchange
One of the hurdle faced during conscioius sedation is excessive sedation which can lead to hypoventilation and hypoxia. THRIVE can be used as an alternative. Thrive is a physiological mechanism for oxygenating and ventilating patients who have diminished or absent respiratory effort. Apnoeic ventilation is established by using THRIVE technique.
Uses of thrive:
- Reduced oxygen reserve
- Procedural sedation
- Difficult airway
- Shared airway.
CONCLUSION:
Proper knowledge, skills and ensuring the availability of equipments is the key to increase the safety of the patient. With the development of MAD administration of drugs made much more easier and less invasive. And nowadays THRIVE can be considered as one of the alternatives for conscious sedation. Conscious sedation offers quick recover and return to everyday activities soon after the procedure.
REFERENCE:
Conscious Sedation in Dentistry – Arpita Kapur and Vinay Kapur1.Ann Maxillofac Surg. 2018 Jul-Dec; 8(2): 320–323.
Inhalation Conscious Sedation with Nitrous Oxide and Oxygen as Alternative to General Anesthesia in Precooperative, Fearful, and Disabled Pediatric Dental Patients: A Large Survey on 688 Working Sessions Angela Galeotti, 1 Annelyse Garret Bernardin, 1 Vincenzo D’Antò, 1 Gianmaria Fabrizio Ferrazzano, 2 Tina Gentile, 1 Valeria Viarani, 1 Giorgio Cassabgi, 1 and Tiziana Cantile
Conscious Sedation With Sevoflurane Anaesthesia Nicola Ross, Anaesthetic RegistrarNatalie Drury, Anaesthetic Registrar, St. James’s University Hospital.
 Dr. Karthik Raja
Dr. Karthik Raja  Dr. Nivetha Ganasundara Sureshkumar
Dr. Nivetha Ganasundara Sureshkumar
{kind=link}