Abstract
Smile is an emotion, an expression of happiness and love. An aesthetic set of dentition comprehends a beautiful smile. Aesthetic teeth help a person exhibit their smile with confidence. As clinicians, we aim at arranging the aesthetic components systematically to provide a person with a pleasing appearance and a vibrant smile. In this article, we present 2 case reports which were treated with different approaches and careful treatment planning to bring about the desired result of an aesthetic smile. In these cases, we have only worked on their dental components based on the facial components and have not made any facial changes.
Introduction
Aesthetics, or esthetics, is a branch of philosophy that deals with the nature of beauty and taste, as well as the philosophy of art. Cosmetic Dentistry or Aesthetic Dentistry plays a vital role in enhancing a person’s smile. Aesthetic Dentistry comprises of various branches of Dentistry which Conservative Dentistry, Endodontics, Orthodontics, Prosthodontics and Periodontics. Smile Designing is the concept of designing a smile based on the principles of facial and dental aesthetics, the needs of the patient and the possibility of executing the design using the various treatment options available. The end result should be aesthetic as well as should help the patient benefit functionally.
The key to Smile Designing is proper diagnosis and documentation. To begin with, a set of clear photographs and diagnostic models are made. The patient’s functional status, the bite, occlusion, space and scope available for treatment are all assessed. The records are then transferred digitally and worked on for designing.
Facial analysis
Analysis and evaluation of both the facial and dental components is the primary principle of Smile Designing (1). The facial components include the hard and soft tissues of the face. Facial corrections may be achieved by including Orthognathic surgery or plastic surgery into the treatment plan. The best facial and dental beauty is achieved by an aesthetic approach to patient care (2). The shape of the face can be identified as square, tapering, ovoid or square tapering. The relationship of the maxilla to the mandible can be assess with the profile of the patient as straight, convex or concave. In clinical practice, unless and until absolutely required, we do not engage in surgical correction of the face and restrict ourselves to smile correction based on the facial components.
The two major components that play a major role in smile correction are the interpupillary line and the lips. From the frontal picture of the patient, the face is analysed based on the following lines. (3)
1. Face is divided into 3 areas horizontally which are meant to be 
equal for an aesthetic face (Fig.1)
a. Glabella (hairline) to Nasion
b. Nasion (Centre point of the eyebrows) to Subnasale
c. Subnasale (Base of the nose) to Menton (Base of the chin)
- The lower 3 rd of the face is further broken down into upper 1/3 and lower 2/3 by a line along the junction of the lips
2. Face is divided into 5 areas vertically, which are also considered to be equal 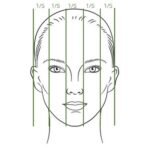
in an aesthetic face (Fig. 2)
a. Lines along the outer border of the face (bilateral)
b. Lines along the outer canthus of the eyes (bilateral)
c. Lines along the inner canthus of the eyes which are
to coincide with the outer margin of the ala of
the nose (bilateral)
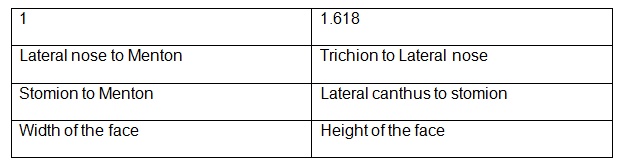
3. Golden proportion
The Golden Proportion of 1:1.618 comes into play in the facial measurements as well as the dental measurements for smile designing. (Table 1) (4)

Table 1 :
Dental Components
1. Relationship of the teeth to the facial structures
a. Facial midline and dental midline to coincide
b. Interpupillary line to coincide with the occlusal plane
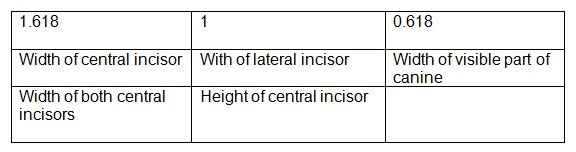
2. Golden proportion (Table 2) (5) applies to the maxillary anterior teeth (Fig.3)
3. Golden rectangle is formed by drawing a box along the outer margins of both
the central incisors
Based on these criteria, the final design is arrived at digitally the various treatment options are weighed based on minimal procedures, treatment duration, preservation of dental structures and most of all, the ease of execution for both the patient and the clinician.
Case Report 1 :
 A 45 year old lady presented with a chief complaint of an unaesthetic smile with chipped crowns and a gummy smile. On clinical examination, she had zirconia crowns on the maxillary anterior teeth (13,12,11,21,22,23), grossly decayed left maxillary second premolar and first molar (25, 26), an implant and crown replacing the right maxillary first molar (16) and a metal ceramic crown replacing the second molar (17). The mandibular arch had a 3unit metal ceramic bridge replacing the right first molar (45,46,47) and a dislodged bridge on the left side with an underlying second premolar root stump (35), a prepared second molar (37). The patient had a severe deep bite, with no visibility of the mandibular anterior teeth and also had severe attrition of the mandibular incisors. (Fig. 4)
A 45 year old lady presented with a chief complaint of an unaesthetic smile with chipped crowns and a gummy smile. On clinical examination, she had zirconia crowns on the maxillary anterior teeth (13,12,11,21,22,23), grossly decayed left maxillary second premolar and first molar (25, 26), an implant and crown replacing the right maxillary first molar (16) and a metal ceramic crown replacing the second molar (17). The mandibular arch had a 3unit metal ceramic bridge replacing the right first molar (45,46,47) and a dislodged bridge on the left side with an underlying second premolar root stump (35), a prepared second molar (37). The patient had a severe deep bite, with no visibility of the mandibular anterior teeth and also had severe attrition of the mandibular incisors. (Fig. 4)
Preoperative diagnostic models, radiographs and photographs were made. The smile was analysed as per the principles of smile designing, based on the facial and dental components. A design was created using the principles of smile designing and a template was created. This design was discussed with the patient and a wax pattern was prepared on the diagnostic model and the final treatment plan was decided. The patient also needed correction of the deep bite to enhance retention of the crowns and bridges. The teeth with good structure and the implant crown were left untouched in order to keep maximum natural tooth structure intact.
 The old crowns and bridges were removed. The root stumps were extracted under local anesthesia, intentional root canal treatment was done for the teeth to be used as abutments. Heat cure acrylic bridges with a raised bite was fixed. The patient was given 2 months to get adapted to the new bite. (Fig.5)
The old crowns and bridges were removed. The root stumps were extracted under local anesthesia, intentional root canal treatment was done for the teeth to be used as abutments. Heat cure acrylic bridges with a raised bite was fixed. The patient was given 2 months to get adapted to the new bite. (Fig.5)
Gingivectomy was done for the maxillary anterior teeth according to the gingival margin of the canine. Temporary crowns were removed and preparations were refined for the final crowns and bridges. The final restorations which consisted on zirconia crowns for the maxillary anterior teeth and porcelain fused to metal restorations for the posterior teeth were prepared based on the final design and delivered to the patient. (Fig. 6)
Dental esthetics, bite correction, correction of the gummy smile and a harmonious occlusion were achieved in this case through smile designing. (Fig. 7)

Case report 2:

This was a case where smile designing was done for a functional reason and was treated with orthodontics.
A 41 year old lady reported with a chief complaint of heavy calculus deposits around the maxillary and mandibular anterior teeth, irregularly placed maxillary and mandibular teeth with cross bites, bone loss in relation to the mandibular anterior teeth with mobility of different grades. (Fig. 8)
The goal of treatment in this patient was to help her maintain good oral hygiene and enhance her periodontal status. This patient was not fit for heavy orthodontic forces due to her poor bone health and also for arch expansion using open coil springs. Hence, the right maxillary lateral incisor and the right mandibular central incisor were extracted to create space. She had a 3 unit metal ceramic bridge on the mandibular posterior teeth, which was not disturbed as it was intact and we had decided not to tamper the occlusion.
 Metal braces were bonded on her teeth. Bite blocks were placed on the maxillary molars to relieve the cross bite, leveling and alignment was completed. Maximum space closure was achieved. We were still left with 3.5 mm on the maxillary anterior teeth, as we had achieved ideal overjet and overbite. Aesthetic light cure composite fillings were done to close the spaces, the right maxillary canine was reshaped to mimic the lateral incisor, and fixed lingual retainers were bonded on the maxillary and mandibular anterior teeth. Regular periodontal follow-ups were done and the gingival status was monitored. (Fig.9)
Metal braces were bonded on her teeth. Bite blocks were placed on the maxillary molars to relieve the cross bite, leveling and alignment was completed. Maximum space closure was achieved. We were still left with 3.5 mm on the maxillary anterior teeth, as we had achieved ideal overjet and overbite. Aesthetic light cure composite fillings were done to close the spaces, the right maxillary canine was reshaped to mimic the lateral incisor, and fixed lingual retainers were bonded on the maxillary and mandibular anterior teeth. Regular periodontal follow-ups were done and the gingival status was monitored. (Fig.9)
An aesthetic smile was delivered to this patient which also enhanced her ability to maintain her oral hygiene very well. (Fig. 10)

Conclusion:
Dental aesthetics forms an important aspect of facial beauty. Smile designing and aesthetic dentistry help in enhancing a person’s smile, confidence and beauty. The key point to be kept in mind during smile designing is preservation of maximum tooth structure, dental component correlating with the facial components and most importantly achieving a harmonious occlusion and restoring function.
References
1. Kokich VO, Jr, Kiyak HA, Shapiro PA. Comparing the perception of Dentist and Lay people to altered Dental Esthetics. J Esthet Dent. 1999;11:311–24.
2. Goldstein RE. Chicago, US: Quintessence Publication; 1997. Change your smile
3. An approach to structural facial rejuvenation with fillers in women R. Fitzgerald et al. / International Journal of Women's Dermatology 5 (2019) 52–67
4. Evaluation of Facial Beauty Using Anthropometric Proportions Jovana Milutinovic, Ksenija Zelic and Nenad Nedeljkovic, February 2014 The Scientific World Journal 2014(2):428250
5. The Golden Proportion Tripuravaram VK Reddy, Sihivahanan Dhanasekaran, Journal of Operative Dentistry and Endodontics, July-December 2017;2(2):79-83
 Dr. Rakesh. U
Dr. Rakesh. U Dr. Kirthana Rao
Dr. Kirthana Rao