Abstract :
We report a case of a young female who presented to emergency department with rapidly developing visual deficits in the form of hemianopia. Her NIHSS score was 2/42. She was thrombolysed with tenecteplase and she showed good improvement in her neurological symptoms. Thrombolysis in very low NIHSS Score (0/1) is associated with increased risk of bleed and lower rate of excellent outcome. Thrombolysis in low NIHSS score (2-5) is associated with early neurological deterioration but with excellent outcome at 3 months. This patient is presented for the excellent neurological outcome she had because of thrombolysis, though her NIHSS score was low.
Case report :
A 39-year lady presented to emergency department of Kauvery hospital with H/O sudden onset giddiness associated with Right eye blurring of vision. She also had headache and 1 episode of non-projectile and non-bilious vomiting. The patient was initially evaluated at an Eye hospital, and she was diagnosed with right eye Homonymous Hemianopia with normal fundus.
Past medical history:
She is a known case of Migraine with frequent episodes ,2-3 episodes/week.
On initial evaluation at ER:
Airway:
Patent and self-maintained
Breathing:
RR 18/min, SPO2 99% in RA, B/L Air entry equal NVBS
Circulation:
PR 90/min, BP 130/80mmhg,
CVS- S1S2 normal, no murmur, JVP-Normal,
P/A- Soft, non-tender, no organomegaly, bowel sounds heard
Disability:
GCS was 15/15, CBG 111mg/dl
Right eye homonymous hemianopia
B/L Pupil 3mm RTL, no nystagmus, HMF/CN- normal,
speech – normal, Power all 4 limbs 5/5, DTR++ all 4 limbs, EOM- No Gaze Palsy, B/L Plantar reflex+.
Exposure:
Temp – nil significant
Her NIHSS Score was 2/42. She was rapidly mobilised for MRI.
Her DWI images (Fig:2) revealed diffusion restriction in left occipital and posterior temporal lobe(PCA territory).
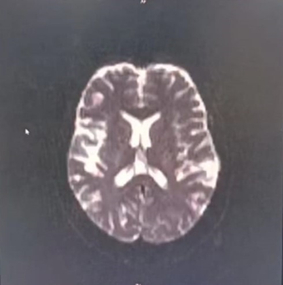
Fig:1- T2 MRI BRAIN Normal
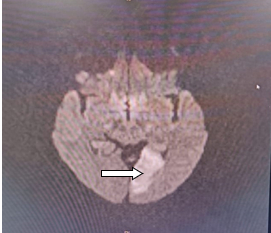
Fig:2 DWI – occipital lobe Diffusion Restricted
In view of young age and CVA in window period and in spite of low NIHSS score it was decided to thrombolyse the patient weighing the risk benefit ratio. After written consent she was given a dose of Tenecteplase (0.25mg/kg) (16mg) in MRI console. After 24 hours of thrombolysis repeat CT Brain done showed no evidence of bleed (Figure:3).Patient reviewed after a week and her visual field had improved Significantly.

Figure 3 . Post thrombolysis CT brain showing no haemorrhage
DISCUSSION:
Posterior cerebral stroke is a common cause of homonymous hemianopia and other neurological deficit and associated with more proximal ischemia in vertebrobasilar circuit.
Symptoms associated with PCA stroke like diplopia, visual field defect, dysphagia, vertigo, alteration in consciousness, memory impairment or reading difficulty may help us to understand the location of stroke.
1.Why PCA stroke cause homonymous hemianopia?
Unilateral infarction of occipital lobe causes contralateral homonymous hemianopia with macular sparring. Calcarine cortex is supplied by posterior cerebral artery.
PCA has four segment P1 to P4 (figure 4). Proximal obstruction in PCA will cause infarct in thalamus, posterior temporal lobe and occipital lobe . Distal obstruction will cause pure occipital lobe infarct. (Figure 5) FIGURE 4: PCA branches

2. How common is hemianopia in PCA stroke?
Studies revealed, with pure PCA stroke 22% presented with hemianopia and 17% with Quandrantanopia. The most common impairment were motor paralysis (65%) and followed by visual defect (54%) , confusion or agitation (45%)
Mechanism of PCA stroke are variable and include large artery disease, Small artery disease, atherothrombosis of PCA, BA, and VA embolism.
3. Why thrombolysed with low NIHSS score?
PCA strokes may be underestimated by NIHSS points, when compared to anterior circulation strokes. In this patient with contralateral homonymous hemianopia has only 2 NIHSS points. While patient has a significant infarct in the occipital cortex and thus daily life will be affected drastically. Studies have proven the beneficial effect of thrombolysis in PCA stroke with Low NIHSS to prevent morbidity.
4. Prognosis and treatment of hemianopia in PCA stroke?
Mortality associated with isolated PCA strokes is low, therefore prognosis is good.
CONCLUSION:
PCA territory stroke can present with subtle manifestation like hemianopia. If left untreated it can lead to major PCA infarct involving thalamus and brainstem stroke from basilar obstruction. Though NIHSS score may be low and the presentation is subtle PCA strokes can be dangerous. Thrombolysis in spite of low NIHSS score results in better functional outcome and also prevents mortality as in this case.
REFERENCE
- Zhang, Xiaojun MD; Kedar, Sachin MD; Lynn, Michael J MS; Newman, Nancy J MD; Biousse, Valérie MD. Homonymous Hemianopia in Stroke. Journal of Neuro-Ophthalmology 26(3):p 180-183, September 2006. | DOI: 10.1097/01.wno.0000235587.41040.39
- Appelros P, Karlsson GM, Seiger A, Nydevik I. Prognosis for patients with neglect and anosognosia with special reference to cognitive impairment. Journal of Rehabilitation Medicine. 2003 Nov;35(6):254-258. DOI: 10.1080/16501970310012455. PMID: 14664314.
- Natale N, Petit R, Champane J, Rodriguez C, Ladna J, Savu C. A Rare Presentation of Posterior Cerebral Artery Stroke With Monocular Hemianopia After Diesel Exposure. Cureus. 2021 May 12;13(5):e14977. doi: 10.7759/cureus.14977. PMID: 34131529; PMCID: PMC8195542.
 Dr. Sangavi
Dr. Sangavi Dr. Aslesha Vijaay Sheth
Dr. Aslesha Vijaay Sheth Dr. Vidya Saketharaman
Dr. Vidya Saketharaman