65-year-old male k/c/o carcinoma vocal cord which was diagnosed 10 months back for which he received radiotherapy and underwent microlaryngeal excision of laryngeal papilloma. Then he had h/o voice change for last 2 months and PET CT revealed SUBGLOTTIC GROWTH for which he was posted for Direct Laryngoscopy + biopsy.
PREOPERATIVE PLANNING:
- Routine investigations were done and blood investigations were found to be within normal limits. ECG- NSR; ECHO- N LV.
- After discussion with surgeon, plan of anaesthesia and risk associated with anaesthesia and procedure were clearly explained to patient and attender with written consent.
- NPO guidelines were followed.
- Pre-medication – INJ PANTOPRAZOLE 40 MG IV INJ PALANOSETRON 0.075 MG were given.
INTRAOPERATIVE MANAGEMENT:
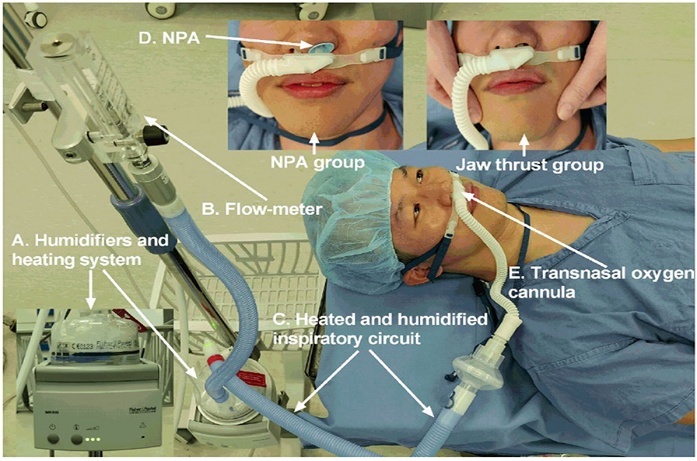
- Patient was positioned supine and ASA Standard monitors were attached and nasal cannula of THRIVE was placed.
- Preoperative saturation – 98% under room air.
- Preoxygenation was started with 100% oxygen at a rate of 20 l/min for 3 minutes.
- Intravenous anaesthesia was started with Inj midazolam 1 mg; Inj fentanyl 100mcg; Inj propofol 80 mg.
- Oxygen flow rate of THRIVE was increased to 50-60 l/min, once the patient lost consciousness and jaw thrust was used to maintain airway patency until insertion of surgical laryngoscope.
- After establishing adequate bag and mask ventilation, INJ atracurium 15mg was given.
- Anaesthesia was maintained with TIVA using propofol in titrated doses.
- Oxygen saturation was maintained for 15 minutes, then patient had desaturation {spo2 <90% }, bag and mask ventilation was done intermittently to achieve oxygenation once during the 45 mins duration of procedure.
- Specified THRIVE equipment delivered high flow nasal oxygen varied from 10-60 l/min with an FI02 of 1 throughout the procedure.
- Neuromuscular blockade was reversed with neostigmine.
- Jaw thrust with bag-mask ventilation was commenced until return of spontaneous respiration.
- The patient was shifted to the recovery room, maintaining his own airway and got discharged on the same day.
DISCUSSION:
- As sharing an airway between the surgeon and the anaesthesiologist is a difficult and challenging task, apnoeic oxygenation technique is a reliable method of maintaining oxygenation during short upper airway procedures.
- Upper airway surgeries can be performed under endotracheal tube or tubeless technique such as jet ventilation, intermittent apnoeic ventilation and THRIVE.
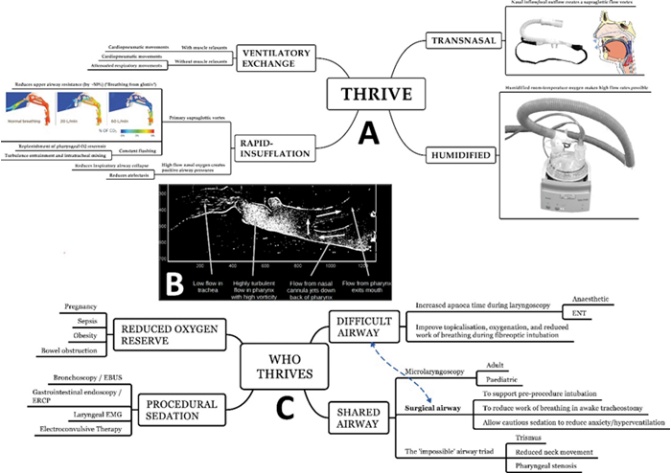
THRIVE – TRANSNASAL HUMIDIFIED RAPID INSUFFLATION VENTILATORY EXCHANGE:
- A novel technique which utilizes high flow [60-70l/min] 100%oxygen, which is humidified, warmed to 37 degree C and administered via nasal cannula.
- Follows a physiological phenomenon of Aventilatory mass flow for providing apnoeic oxygenation
PHYSIOLOGICAL BENEFITS
- INCREASE IN APNOEIC TIME AND CARBON DIOXIDE CLEARANCE :
THRIVE via HFNC has extended the apnoeic window by up to 65 minutes, while reducing the rise in rate of CO2.
- GAS CONDITIONING -HEATING AND HUMIDIFICATION:
By warming and humidifying the gas, high flow reduce the metabolic rate of respiration. Humidification prevent drying of secretions and thus reduce mucus plugging, atelectasis and hypoxia.
- FIXED FI02 DELIVERY AND DEAD SPACE WASHOUT:
It implies minimal room air entrainment.
- POSITIVE AIRWAY PRESSURE
HFNO supplies positive airway pressure of approximately 1cmH2O per 10l/min flow rate.
BENEFITS IN ANAESTHESIA PRACTICE
- DIFFICULT AIRWAY MANAGEMENT
This technique affords the luxury of time to think and utilize the other method of securing the airway while maintaining oxygenation and reduces the morbidity. One should be aware that this is not applicable in complete upper airway obstruction.
- AIRWAY MANAGEMENT IN OBESE AND PREGNANT PATIENTS
Both have risk for aspiration and desaturation, this technique is used for preoxygenation to decrease the apnoeic period. Used as an adjuvant to assist alveolar recruitment post extubation.
- TUBELESS FIELD SURGERY
To provide an unobscured surgical field while maintaining oxygenation and anaesthesia during airway procedures including upper airway and larynx such as vocal cord biopsy, balloon dilatation, subglottic stenosis, bronchoscopy, endoscopy.
- In this technique patient can be spontaneously breathing or apnoeic with full muscle relaxation, while anaesthesia is maintained with TIVA.
- It prolongs the safe apnoea time and has low risk for barotrauma. Prevents ETT related injury, avoids vocal cord movement and interruptions of intermittent intubation.
- RESPIRATORY SUPPORT DURING PROCEDURAL SEDATION
Used in conscious sedation procedures such as bronchoscopy , colonoscopy, gastroscopy where supplemental oxygen is required.
LIMITATIONS:
Hypercapnia is a valid concern as monitoring of end tidal co2 throughout the procedure is difficult.
CONCLUSION:
THRIVE has improved our practice and patient safety in difficult airway. Combination of THRIVE with TIVA offers a good alternative to conventional anaesthesia with microlaryngeal tubes and jet ventilation in short airway procedures.
REFERENCES:
- 1 May 2018 | Reza Nouraei, James Richard Shorthouse, James Keegan, Fran Haigh, Kate Heathcote, Anil Patel, Michael Girgis | ENT, Head and Neck, Laryngology / Swallowing / Voice
- Bharathi MB, Kumar MRA, Prakash BG, Shetty S, Sivapuram K, Madhan S. New Visionary in Upper Airway Surgeries-THRIVE, a Tubeless Ventilation. Indian J Otolaryngol Head Neck Surg. 2021 Jun;73(2):246-251. doi: 10.1007/s12070-021-02491-2. Epub 2021 Mar 30. PMID: 34150599; PMCID: PMC8163920.
 Dr Velmurugan Desingh
Dr Velmurugan Desingh
Head of the Department,
Department of Anaesthesiology
Kauvery Hospital, Chennai
 Dr S. Dhiveya
Dr S. Dhiveya
Second Year DNB Resident,
Department of Anesthesiology,
Kauvery Hospital, Chennai