Effectiveness of tactile-spatial oriented approach based paediatric occupational therapy intervention for children with Infantile Hemiplegia
Mahendran. M*
Paediatric occupational therapist, Kauvery hospital, Unit of HAMSA Rehab for Kids, Tamil Nadu, India-620001
*Correspondence: Maherichy987@gmail.com
Abstract
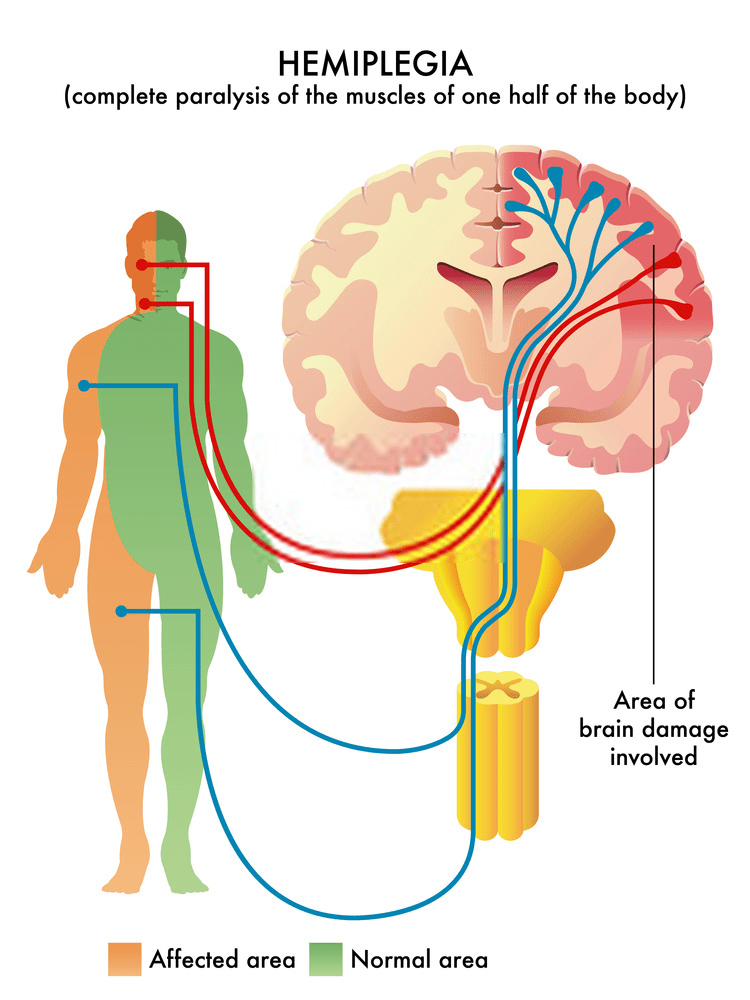
Background: Infantile hemiplegia refers to brain injuries that occur in either high-risk infants, leading to hemiplegia or total paralysis of one side of the body, including the upper and lower extremities. The main purpose of this article is to provide valuable information to paediatric occupational therapists about Tactile-spatial Oriented Approach and treatment alternatives for patients with infantile hemiplegia.
Objective: To assess the functionality of the affected upper and lower limb in infants diagnosed with hemiplegia aged between 0 and 2 years after applying Tactile-spatial Oriented Approach Therapy.
Methods: This was a prospective case study. A Tactile-spatial Oriented Approach protocol was applied for 3 Months, with one hour of restraint (activities not engaging for unaffected side) per day. The study variables included the quality of functional ability of the upper limb, recurrent use, participation of the affected upper limb in self-care and unstructured activities, active joint position, hand grasp–release action, hand grasp strength, supination, and extension elbow movements (tactile-vestibular oriented). Four measurements were performed to assess functional ability based on the Functional Status Score (FSS) and activity based configurational developmental checklist (ABCD-C).
Results: The subject was an infant with moderate manual, activity based configurational developmental checklist (ABCD-C). Statistically significant differences were detected in all studied variables (p < 0.001) between the pre-treatment and post-treatment results (12 weeks), except for upper limb dressing and putting on lower body dressing. In the 8–12-week period, the changes were statistically extremely significant, except for protective extension, grasp strength, grasp–release, and all functional variables (level of functionality and participation of the patient’s upper limbs) in the FSS Evaluation (p < 0.0001). The greatest increase occurred in muscle tone spontaneous use from pre-assessment to post-assessment (p = 0.001), reaching 88.87% active participation in bimanual sensory tasks. The quality of movement of the upper limb exhibited significant improvement due to the increase in dissociated movements and range of motion (p = 0.0702).
Conclusion: A Tactile-spatial Oriented Approach (50 hours) l increased the functionality of infants diagnosed with hemiplegia between birth and 1 year of age with moderate activities ability.
Key words: Paediatric Occupational Therapy; Tactile-spatial Oriented Approach; quality of movement activities; Infantile Hemiplegia
Introduction
Hemiplegia in infants is now recognized as a significant cause of morbidity and mortality. The developmental differences between hemiplegia in infants and adults present unique challenges for its recognition and treatment in infants. The condition is relatively rare in infants, leading to frequent under-recognition and delayed diagnosis. The causes of infant hemiplegia are numerous, with no single predominant risk factor. A variety of conditions can lead to cerebral infarct or haemorrhage in infants, and each case requires a careful and informed diagnostic approach to identify the underlying mechanism and cause.
Increased awareness of infant hemiplegia can lead to more rapid medical attention. With faster diagnosis, future treatment options may include newer thrombolytic and neuroprotective agents. To determine the effectiveness of antithrombotic and other occupational /physical therapies in paediatric patients with hemiplegia, large multicentre collaborative intervention trials are necessary. Although hemiplegia is rare in infants, its effects can significantly, impact a child’s development and result in a lifelong burden of illness. Therefore, developing specific diagnostic and paediatric occupational therapeutic approaches for these conditions is crucial.
To better understand the application of a tactile-spatial oriented approach in paediatric occupational therapy for infants with infantile hemiplegia and functional ability difficulties, population-based studies are needed. These studies should investigate the incidence, etiology, risk factors, and outcomes of infantile hemiplegia and cerebrovascular disease. This study was conducted to analyze the epidemiological and clinical profiles, etiologic factors, risk factors, and disabilities associated with hemiplegia in infants.
Aim and objectives
Aim
The aim of this study was to assess tactile-spatial oriented approach for children with Infantile Hemiplegia.
Objectives
- To measure the functional ability assessment based on Functional Status Score (FSS).
- To evaluate the client developmental goal of OTs implementations among Infantile Hemiplegia using activity based configurational developmental checklist (ABCD-C).
- To evaluate the occupational performance problems, concerns and issues, interview the client, asking about daily activities in self-care amongst paediatrics using (Wee FIM).
- To evaluate synergic pattern among Infantile Hemiplegia using (UE) Flexor Synergy recovering stages.
Case History: As narrated by his parents, a one-year-old boy had been seemingly healthy until about a month ago when he suddenly developed focal seizures. These seizures were initially managed with consultation and medication from their family doctor. However, he continued to experience sudden fevers two to three times weekly. Eventually, the child developed a high-grade fever, prompting his parents to rush him to a nearby government hospital, where he was admitted to the general ward for two days. On the second day, he experienced his first episode of convulsions and was subsequently referred to a KMC hospital, where he was urgently admitted to the paediatric intensive care unit (PICU). Investigations, including an MRI, were conducted, and the child was diagnosed with infantile hemiplegia. During his stay in the paediatric ICU, he had several seizure episodes, which were managed with medication. This condition led to weakness in his right upper and lower limbs. After a 30-day stay in the ICU, the child was transferred to the general ward. Due to the child’s deteriorating condition and the lack of available occupational therapy treatment, he was referred to the KMC hospital unit of Hamsa rehab for kids Centre for further treatment.
The child was referred for paediatric occupational therapy on Jan 2023. He received therapy six days a week for three months with each session lasting 45 to 50 minutes. The therapy was designed to support his flexor synergy recovery stages and functional abilities. Based on the assessment report and a detailed discussion with his parents regarding his medical history, specific goals were set for his therapeutic tactile-spatial oriented approach intervention program. The therapy included tactile-spatial oriented approach activities, transitioning from unstructured to structured formats, and incorporated Sensory Integration and tactile-spatial oriented approach Therapy. Family members were encouraged to actively participate in the sessions, and a home program was provided to his family to support ongoing therapy efforts.
Methodology
Experimental design: This type of research design use at a problem scientifically by establishing a clear cause and effect of every stage. It also tries to understand the impact of the independent variable on the dependable variable. Often social sciences use it to observe case behaviours and understand the social psychology of human being better.
Research instruments: In this project, the data are collected through structured questionnaire. (Functional Status Score (FSS) Questionnaire: A questionnaire is a schedule consisting of a number of formulated series of questions related to the various aspect of subjects under study. In this method a pre-printed list of questions, arranged in sequences is used to retrieve response from the activity based configurational developmental checklist (ABCD-C). respondent.
Tools for data analysis and interpretation
Bar Diagram (Bar Chart) Explanation: A bar diagram uses rectangular bars to show comparisons among categories. In this context, each bar represents a category of data, such as the pre-intervention and post-intervention values for Infantile Hemiplegia. The height of each bar indicates the value or frequency for that specific category, allowing for a clear comparison between the pre-intervention and post-intervention outcomes.
Sample design: Sample design lay down all the details to be included in the sample. It is a definite plan for obtaining a sample from a given population. The sample technique used was the random sampling. In this type of sampling items for the sample are selected deliberately.
Study population: Outpatient – Case study, KMC hospital, unit of Hamsa rehab for kids, Trichy, Tamil Nadu, India.
Sample size: Sampling is the process of obtaining information about the entire population by examining only a part of it. Due to shortage of time researcher found it difficult to approach each case personally. I have collected the data from pilot study. The samples were collected using simple random sampling method.
Table1: Paediatric Occupational Therapy intervention: The Occupational Therapy intervention protocol is depicted in follows
| Problem identified | Goal | Treatment strategy | Intervention technique’s |
|---|---|---|---|
| Functional ability | To integrative muscle tone and posture | activity based configurational developmental Approach | 45-degree swing |
| 90-degree swing | |||
| Combination of 90+45-degree swing | |||
| Head/neck control | To enhance head and neck control | Tactile-spatial Oriented Approach (centre of gravity based) | Prone on position-eye ball tracking |
| Head control in prone activities with a wedge | |||
| Full body extension and supine lateral rolls with flat swing | |||
| Chair swing activities | |||
| Sensation | To integrative primary sensory components(Touch sense, height fear sense) | Tactile-spatial Oriented Approach (centre of gravity based) | Tactile activities |
| Proprioceptive activities | |||
| Vestibular activities | |||
| Oro motor | Improve muscle strength | Oro-motor-muscular Facilitation | Tongue thrust, tapping, clock anti clockwise-facilitation (face muscles) |
| Hand function- Flexor Synergy | Improve Hand function | activity based configurational developmental Approach | Affected side-involving activities maximum as per extensor movement therapy protocol |
Outcome measure
Table 2: Characteristic of data pre-post-evaluation- Modified Ashworth scale (MAS)
| Characteristic of data-Unpaired t-test | pre-test evaluation (MAS) | post-test evaluation (MAS) |
|---|---|---|
| Mean | 4.43 | 0.71 |
| standard deviation | 0.53 | 0.49 |
| Sample size | 1 | 1 |
| standard error (SE) means | 0.20 | 0.18 |
| 95% confidence interval difference | 3.12 | 4.31 |
Table 2; data shows (MAS) pre-post-test evaluation scores of all mono subject, mean values are 4.43 and 0.71, respectively standard deviation 0.53 and 0.49 respectively sample size, standard error of mean 0.20 and 0.18, the mean of pre control and experimental 95% 01confidence interval of this difference 3.12 and 4.31, respectively.
Table 3:‘t’ test between characteristics of data pre-post-evaluation- Modified Ashworth scale (MAS)
| One-Sample Statistics | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Type | N | Mean | Std. Deviation | Std. Error Mean | t | df | Sig. (2-tailed) | Mean Difference | 95 % CI Lower | 95 % CI Upper |
| PRE MAS | 7 | 4.43 | .535 | .202 | 21.920 | 6 | .000 | 4.429 | 3.93 | 4.92 |
| POST MAS | 7 | .71 | .488 | .184 | 3.873 | 6 | .008 | .714 | .26 | 1.17 |
Graph 1: Mean of Pre control and pre-experimental groups of evaluation -Modified Ashworth scale (MAS)
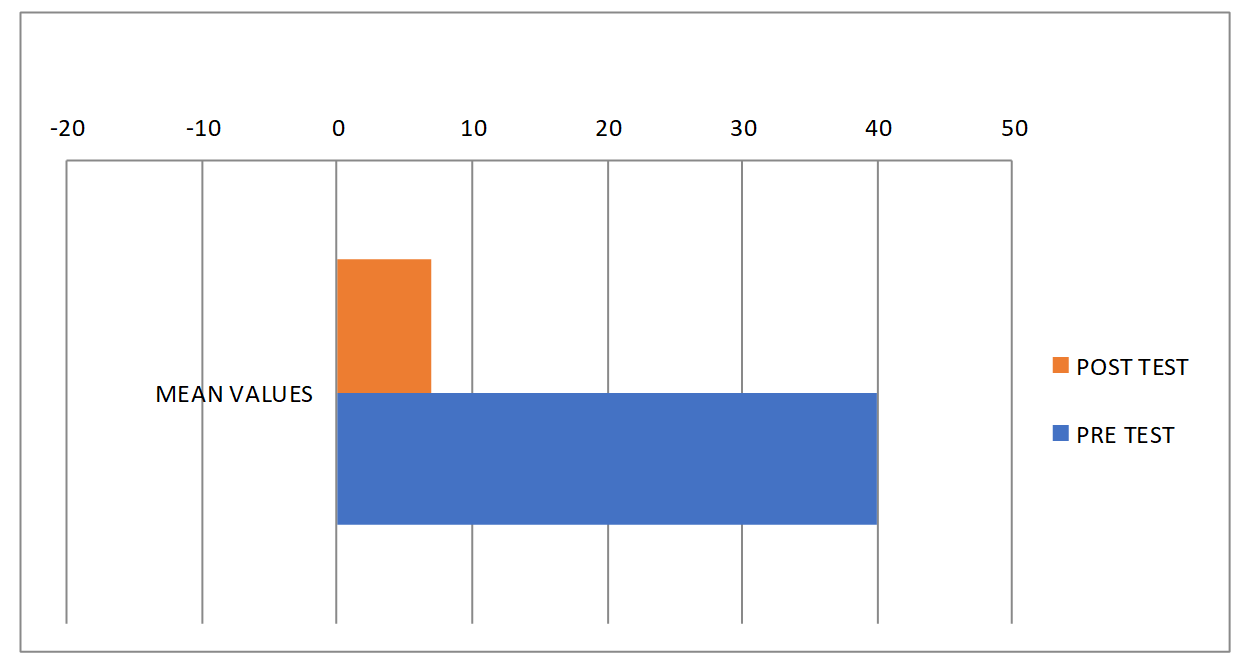
Table 4: Characteristic of data pre-post-evaluation- FSS
| Characteristic of data-Unpaired t-test | pre-test evaluation (FSS) | post-test evaluation (FSS) |
|---|---|---|
| Mean | 2.00 | 5.83 |
| standard deviation | 0.00 | 0.38 |
| Sample size | 1 | 1 |
| standard error (SE) means | 0.00 | 0.09 |
| 95% confidence interval difference | -4.02 | -3.65 |
Table 4; data shows (FSS) pre-post-test evaluation scores of all mono subject, mean values are 2.00 and 5.83, respectively standard deviation 0.00 and 0.38 respectively sample size, standard error of mean 0.00 and 0.09, the mean of pre control and experimental 95% 01confidence interval of this difference -4.02 and -3.65, respectively.
Table 5:‘t’ test between characteristics of data pre-post-evaluation- Functional status score (FSS)
| One-Sample Statistics | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Type | N | Mean | Std. Deviation | Std. Error Mean | t | df | Sig. (2-tailed) | Mean Difference | 95 % CI Lower | 95 % CI Upper |
| Pre FSS | 18 | 2.00 | .000a | 0.000 | ||||||
| Post FSS | 18 | 5.83 | .383 | .090 | 64.537 | 17 | .000 | 5.833 | 5.64 | 6.02 |
Graph 2: Mean of characteristics of data pre-post-evaluation- Functional status score (FSS)

Table 6: Characteristic of data pre-post-evaluation- Sensory profile (SP-2)
| Characteristic of data-Unpaired t-test | pre-test evaluation (SP-2) | post-test evaluation (SP-2) |
|---|---|---|
| Mean | 39.71 | 21.43 |
| standard deviation | 20.23 | 14.01 |
| Sample size | 1 | 1 |
| standard error (SE) means | 5.40 | 3.74 |
| 95% confidence interval difference | 1.50 | 27.50 |
Table 6; data shows (SP-2) pre-post-test evaluation scores of all mono subject, mean values are 35.93 and 21.43, respectively standard deviation 19.06 and 14.01 respectively sample size, standard error of mean 5.09 and 3.75, the mean of pre control and experimental 95% 01confidence interval of this difference 1.50 and 27.50, respectively.
Table 7: ‘t’ test between characteristics of data pre-post-evaluation- Sensory profile (SP-2)
| One-Sample Statistics | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Type | N | Mean | Std. Deviation | Std. Error Mean | t | df | Sig. (2-tailed) | Mean Difference | 95 % CI Lower | 95 % CI Upper |
| Pre -C Sensory Profile-2 | 14 | 39.71 | 20.239 | 5.409 | 7.342 | 13 | .000 | 39.714 | 28.03 | 51.40 |
| Post C- Sensory Profile-2 | 14 | 21.43 | 14.015 | 3.746 | 5.721 | 13 | .000 | 21.429 | 13.34 | 29.52 |
Graph 3: Mean of Pre control and pre-experimental groups of evaluation -Sensory profile (SP-2)
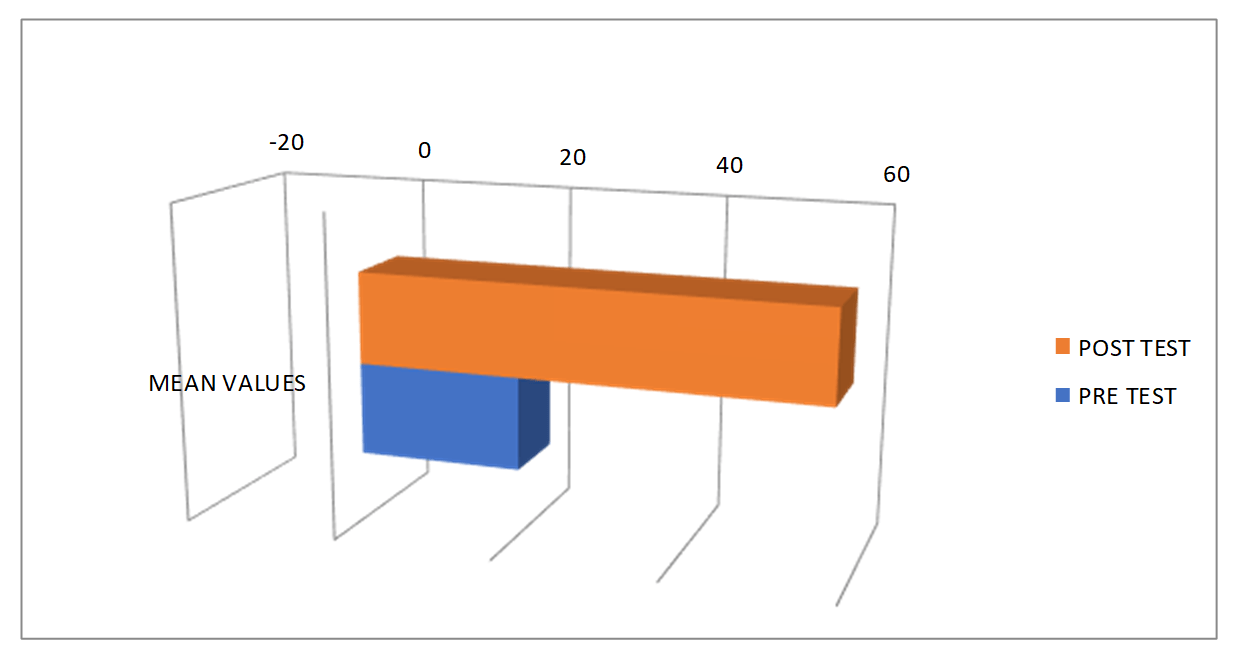
Table 8: Characteristic of data pre-post-evaluation- Range of motion (ROM)
| Characteristic of data-Unpaired t-test | pre-test evaluation (ROM) | post-test evaluation (ROM) |
|---|---|---|
| Mean | 21.00 | 47.40 |
| standard deviation | 17.10 | 22.50 |
| Sample size | 1 | 1 |
| standard error (SE) means | 7.65 | 10.06 |
| 95% confidence interval difference | -55.55 | 2.75 |
Table 8; data shows (ROM) pre-post-test evaluation scores of all mono subject, mean values are 21.00 and 47.40, respectively standard deviation 17.10 and 22.50 respectively sample size, standard error of mean 7.65 and 10.06, the mean of pre control and experimental 95% 01confidence interval of this difference -55.55 and 2.75, respectively.
Table 9: ‘t’ test between characteristics of data pre-post-evaluation- Range of motion (ROM)
| One-Sample Statistics | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Type | N | Mean | Std. Deviation | Std. Error Mean | t | df | Sig. (2-tailed) | Mean Difference | 95 % CI Lower | 95 % CI Upper |
| Pre-ROM | 5 | 14.00 | 5.477 | 2.449 | 5.715 | 4 | .005 | 14.000 | 7.20 | 20.80 |
| Post -ROM | 5 | 47.40 | 22.501 | 10.063 | 4.710 | 4 | .009 | 47.400 | 19.46 | 75.34 |
Graph 4: Mean of Pre control and pre-experimental groups of evaluation -Range of motion (ROM)

Table 10: Characteristic of data pre-post-evaluation- activity based configurational developmental checklist (ABCD-C).
| Characteristic of data-Unpaired t-test | pre-test evaluation | post-test evaluation |
|---|---|---|
| Mean | 2.80 | 9.40 |
| standard deviation | 0.45 | 0.89 |
| Sample size | 1 | 1 |
| standard error (SE) means | 0.20 | 0.40 |
| 95% confidence interval difference | -7.63 | -5.57 |
Table 10; data shows pre-post-test evaluation scores of all mono subject, mean values are 2.80 and 9.40, respectively standard deviation 0.45 and 0.89 respectively sample size, standard error of mean 0.20 and 0.40, the mean of pre control and experimental 95% 01confidence interval of this difference -7.63 and -5.57, respectively.
Table 6:‘t’ test between characteristics of data pre-post-evaluation- activity based configurational developmental checklist (ABCD-C).
| One-Sample Statistics | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Type | N | Mean | Std. Deviation | Std. Error Mean | t | df | Sig. (2-tailed) | Mean Difference | 95 % CI Lower | 95 % CI Upper |
| Pre-ABCD Checklist | 5 | 2.80 | .447 | .200 | 14.000 | 4 | .000 | 2.800 | 2.24 | 3.36 |
| Post -ABCD checklist | 5 | 9.40 | .894 | .400 | 23.500 | 4 | .000 | 9.400 | 8.29 | 10.51 |
Graph 5: Mean of Pre and post evaluation -activity based configurational developmental checklist (ABCD-C)


Fig (1): shows pre-post-test evaluation master
Discussion
The present study was designed to compare the two treatment modalities, i.e., Tactile-spatial Oriented Approach therapy and activity based configurational developmental Approach activities for reducing spasticity and improving hand function in infantile hemiplegia, to find the effects of these approaches on spasticity of wrist flexors and finger flexors and improvement in hand function in infantile hemiplegia survivors.
Conclusion
Subjects with infantile hemiplegia who undergo Tactile-Spatial Oriented Approach Therapy, particularly those facing functional ability difficulties, show significant improvement. This therapy effectively reduces muscle tone issues and addresses postural problems in these infants. The improvements are achieved through a developmental approach that configures activities to support their specific needs.
Tactile-Spatial Oriented Approach-Based Paediatric Occupational Therapy Intervention plays a crucial role in enhancing participation, improving motor skill development, and facilitating functional performance in both upper and lower extremities for children with infantile hemiplegia. This approach also helps children engage in meaningful day-to-day activities by focusing on tactile-spatial orientation.
By concentrating on the affected side, the Tactile-Spatial Oriented Approach promotes active involvement in recovery and enhances the child’s ability to perform activities. Task analysis within this approach involves understanding the nature of the task and the internal and external factors that either facilitate or impede performance.
Acknowledgments
I would like to extend my sincere gratitude to all those who have contributed to the completion of this study. First and foremost, I thank the children and their families who participated in this research; without their cooperation and commitment, this study would not have been possible.
I am deeply grateful to my colleagues and the staff at Child development centre and HAMSA Rehab for Kids for their unwavering support and assistance throughout the research process. Special thanks to Dr. Meganathan., Dr. Bruno Raju, Dr. Suresh Subramony Venkita for their invaluable guidance and mentorship, which has been instrumental in shaping the direction and quality of this research. I also wish to acknowledge the administrative support Dr G. Balamurali., from the management of Hamsa Rehab, Dr. Manivannan Selvaraj is the Founder and Managing Director of Kauvery Group of Hospitals, Trichy, Tamil Nadu, India. Their facilitation of resources and ethical clearances was crucial for the smooth conduct of this study. Lastly, I express my heartfelt appreciation to S.M. Surya., for their continuous encouragement and understanding during the course of this research. Their support has been a pillar of strength for me.
References
- Alexis Thompson (1890) Microcephaly and infantile hemiplegiaMemories surla microcephalie, gratiolet, journalVol 28 (N.S. Vol8) Pg no 420-444
- Brown, T., & Chien, C.W. (2010). Top-down or bottom-up occupational therapy assessment: Which way do we go?. British Journal of Occupational Therapy, Vol 73(3), pp. 95-97.
- Bundy, A.C., Lane, S.J., & Murray, E.A. (2002). Sensory Integration: Theory and Practice. F.A. Davis Company. This text discusses various therapeutic approaches including activity configurations in pediatric occupational therapy.
- Campbell, W.N., & Egan, M.Y. (2010). Occupational performance measures: In practice. Canadian Journal of Occupational Therapy, Vol 77(1), pp. 22-30. Explores the use of various performance measures, including configurational approaches in therapy.
- Case-Smith, J. (2001). Occupational therapy for children with hemiplegia. Physical & Occupational Therapy in Pediatrics, Vol 21(3-4), pp. 57-76. This article reviews various approaches, including activity configuration, for children with hemiplegia.
- Case-Smith, J., & O’Brien, J.C. (2015). Occupational Therapy for Children and Adolescents. Elsevier Mosby. This book provides comprehensive coverage of pediatric occupational therapy, including activity configurational approaches.
- Cohn, E.S., & Kramer, J. (2007). A conceptual foundation for occupational therapy practice with children. American Journal of Occupational Therapy, Vol 61(6), pp. 681-691.
- V.M.Bishop (1983 )Linguistic impairment after left hemidecortication for infantile hemiplegia? AreappraisalQuarterly journal of experimental psychologyVol 35APg no 199-207
- Hirokazu oguni, kitami hayashi, Norihisa usui, Makkiko osawa, Hiroyuki Shimizu(1998) Startle epilepsy with infantile hemiplegia report of two cases improved by surgeryLippincott -Raven publishers,philadelphia International league against epilepsyVol 39(1)Pg no 93-98
- B. Griffith (1965 )Cerebral hemispherectomy for infantile hemiplegia in the light of the late resultsJ. Neural Neurosurg psychiatryPg no :183-201
- John Mcfie (1961 )The effects of hemispherectomy on intellectual functioning in cases of infantilehemiplegiaJ. Neural. Neurosurg, psychiatVol 24 pgno 240-24.
- Mailloux, Z., & Smith Roley, S. (2010). Sensory Integration Development and Early Intervention. American Occupational Therapy Association. Discusses the role of sensory integration and activity configuration in early intervention.
- Mahendran M, Surya S M., (2023). Application of Short-Concentration Modified Constraint-Induced Movement Therapy for Infantile Hemiplegia with Functional Ability Difficulties: Case Study Tamil Nadu Journal of Public Health and Medical Research, Volume: 3 – Issue:3.,2023PP 63-68
- palomo C Rocio and Garcia -Muro San Jose (2018) Increase in visual motor coordination after applying mCIMT in infantilehemiplegia, Report of a casePediatric dimensionsVol 3(4) pg no 1-5
- Parham, L.D., & Fazio, L.S. (2008). Play in Occupational Therapy for Children. Elsevier Mosby. It highlights the importance of play and activity configuration in therapeutic settings.
- Polatajko, H.J., Davis, J.A., Stewart, D., Cantin, N., Amoroso, B., Purdie, L., & Zimmerman, D. (2007). Specifying the domain of concern: Occupation as core. Canadian Journal of Occupational Therapy, Vol 74(1), pp. 75-88.
- Reed, K.L., & Sanderson, S.N. (1999). Concepts of Occupational Therapy. Lippincott Williams & Wilkins. This book delves into the theoretical underpinnings of occupational therapy practices, including activity configuration.
- Rowland A. Krynauw (1950) Infantile hemiplegia treated by removing one cerebral hemisphereJ. Neural Neurosurg, psychiat,.Vol 13 pg no 243- 267
- Vanitha (2008) Study on profile of hemiplegia in children, govt. Stanley medical college & hospital the Tamil Nadu Dr.M.G.R.Medical university Chennai, India.
- Wilcock, A.A., & Townsend, E.A. (2014). Occupational Justice and Client-Centred Practice: A Dialogue in Progress. Canadian Journal of Occupational Therapy, Vol 81(2), pp. 61-69.
- Wylie McK issock (19530Infantile hemiplegiaProceedings of the Royal Society of medicineVol 46- 431Pg no 37-40.
