Efficacy of early diagnosis and development approaches of paediatric occupational therapy on acute disseminated encephalomyelitis: A case report
M. Mahendran*
Kauvery hospital, Unit of Hamsa Rehab for kids Trichy, Tamil Nadu
*Correspondence: Maherichy987@gmail.com
Abstract
This case study investigates the efficacy of early diagnosis and integrated pediatric occupational therapy approaches in the management of Acute Disseminated Encephalomyelitis (ADEM) in a three-year-old female patient. The study focuses on the development of performance problems in daily activities, employing a prospective case study design with a developmental protocol applied over 8 weeks. The primary outcomes measured include functional ability of the upper limb, recurrent use, participation in self-care and semi-structured activities, active joint position, hand grasp-release action, hand grasp strength, supination and extension elbow movements. The study reports statistically significant improvements in various parameters after the intervention.
Background
The ADEM is a rare neurodegenerative disease of the central nervous system, diagnosed through neuroimaging and based on exclusion. Early diagnosis and pediatric occupational therapy are crucial for successful outcomes. The case involves a three-year-old female with neurological symptoms, including slurred speech, headache, and difficulty swallowing, leading to a diagnosis of ADEM. Medical and occupational therapy interventions were initiated, with the patient showing improvement and eventual discharge after 8 weeks.
Methodology
The study is a prospective case study with a focus on a three-year-old female diagnosed with ADEM. The treatment plan involved a developmental protocol for 8 weeks, with measurements performed before and after the intervention. Various scales and checklists were used to assess muscle tone, sensory components, and functional abilities. The statistical analysis indicated significant improvements in measured parameters post-intervention.
Occupational Therapy Intervention
The occupational therapy intervention utilized a developmental approach, including sensory integration, Rood’s approach, activity configuration therapy, and basic activities of daily living (BADL) training. Specific goals were set for enhancing functional ability, self-care activities, and integrative sensation. Various activities were employed to address muscle strength, hand function, and sensory integration.
Outcome Measures
The outcomes were measured using the Modified Ashworth Scale (MAS) for muscle tone, the Functional Independence Measure for Children (weeFIM), and the Activity-Based Configurational Checklist (ABCD). The results demonstrated statistically significant improvements in MAS grades, weeFIM scores, and ABCD checklist components.
Discussion
The study aimed to determine the efficacy of early diagnosis and integrated pediatric occupational therapy approaches in ADEM cases. The combination of developmental approaches and activity configurational therapy at home was well-accepted and resulted in improved parental competence and child outcomes.
Conclusion
The study concludes that early diagnosis and integrated pediatric occupational therapy approaches significantly contribute to the improvement of functional abilities in ADEM patients. The developmental approach-based therapy and activity configurational therapy positively impacted the child’s daily functions. Occupational therapy analysis emphasizes goal-setting and enhancing hand function for better recovery.
Limitations
The study acknowledges limitations, including the broad scope of the research and the inability to provide detailed case metaphors for direct comparison. The lack of specific details about individual ADEM interventions and variations in activities and settings is also noted.
Aim
The main purpose of this study is to demonstrate the efficacy of early diagnosis and integrated approaches of paediatric occupational therapy on Acute Disseminated Encephalomyelitis.
Objective
To evaluate the development of performance problems and related concerns and issues
To interview the client and ask about daily activities in self-care amongst children with acute disseminated encephalomyelitis (ADEM).
Methods and materials
Settings: Subjects selected from the ADEM Unit of the Rehabilitation Kids for HAMSA (Trichy, India)
Participants: Three-year female baby, with seizure, at second hospitalization.
Methods: Prospective case study. A developmental protocol was applied for 8 weeks, with 45 min of per day. The study variables were functional ability of the upper limb, recurrent use, participation of the upper limb in self-care and semi structured activities, active joint position, hand grasp-release action, hand grasp strength, supination and extension elbow movements. Four measurements were performed, to measure the sensory assessment based on childs sensory profile.
Results
Statistically significant differences were detected in all the studied variables between the pre-treatment and post-treatment Manual muscle testing (MAS), Multimodal therapy (MMT) grades, the Functional Independence Measure for Children( wee FIM) and ABCD Checklist results in the 8 weeks The changes were statistically significant, except for protective extension, grasp strength, grasp-release and all static functional variables effect.
Key-words: Paediatric Occupational Therapy; Developmental Approach; Acute Disseminated Encephalomyelitis; Early management
Introduction
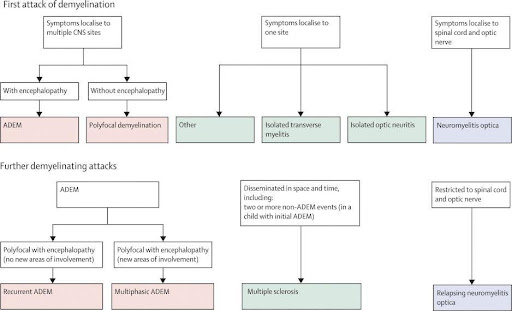
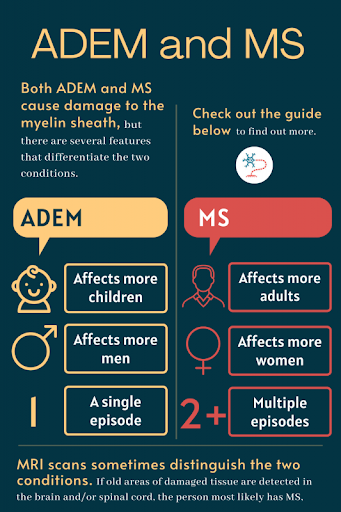
ADEM (Acute Disseminated Encephalomyelitis) is a rare neurodegenerative disease of the central nervous system (CNS). It is a diagnosis of exclusion and is based on neuroimaging (which may be normal at onset). Diagnosis of ADEM is a challenge at first attack. In this case, an adolescent boy recovered well after medical treatment (high dose antibiotics, antiviral and steroid) and paediatric occupational therapy treatment (chronologically sensory integration /Roods /Different Scheme of developmental facilitation and inhibition, activity configurationally therapy and basic activities of daily living (BADL) training).
There are currently no specific biomarkers for the diagnosis of ADEM; therefore, the diagnosis is made after exclusion of other diseases by using clinical and laboratory findings, as well as suggestive neuro radiologic features of other diseases. Early diagnosis and incorporating paediatric occupational therapy approach are the keys to successful outcome.
(Resource: Brenda Banwell, 2007)
Case Presentation
As narrated by parents, the 3-year-old female baby was brought with slurring of speech; headache and difficulty in swallowing with rapid neurological deterioration following fever for 3 days. She was evaluated at emergency. On examination, she was in altered sensorium; tone was increased in upper and lower limb with brisk deep tendon reflexes. Plantar reflexes were rising and cranial nerve examination was normal. No meningeal sign was present. The child had one episode of seizure. She was admitted in the intensive care unit (PICU) KMC hospital. Paediatric occupational therapy treatment was begun three days later
She was in a stable condition after 7 weeks. Gradually she improved and was shifted to Hamsa rehab for kids unit. She was managed by rehabilitation team and Paediatric occupational therapy treatment was started one week later. We began sequentially, with sensory integration, Roods (Roods approach is a neurophysiologic and developmental treatment approach that was developed by Margret Rood to improve tone of muscles, both flaccid and spastic) different schemes of developmental facilitation and inhibition, activity configuration therapy and BADL training. Spatial play activities were introduced. Gradually he improved and was discharged in a stable condition after 8 weeks.
Resource: bio news, Inc.
Methodology
This is a case study.
Before initiating the study, a consent form was given to the parent for participation, with the right to withdraw from the study at any time, if desired by the participant.
The inclusion criteria were a medical diagnosis of ADEM age 3years, lack of activity of the affected upper and lower limb, ability to understand the non-verbal orders given for the execution of tasks and cooperation in their performance.
In the same way, the exclusion criteria were visual problems that prevented the child from carrying out the intervention.
Treatment plan decided was pre and post intervention followed by the application of developmental practices, and primary self-care management followed by weeFIM on a 7-point rating scale.
Upper and Lower extremities: each major joints component was assessed for muscle tone by Modified Aswarth scale (MAS). Upper and lower extremity sensory component was assessed by child sensory profile tool. ABCD checklist component assessed posture, alignment, self-care, and functional ability by Functional Status Score. These scales component, pre and post intervention were statistically analysed.
Paediatric Occupational Therapy intervention-ADEM. The Occupational Therapy intervention protocol is depicted in follows,
Problem identified |
Goal |
Treatment strategy |
Intervention |
| Functional ability | To maximum functional ability | ROODS/NDT | Scapula mobilization activities |
| Trunk rotation activities | |||
| Transfers activities | |||
| Bed mobility activities, Tactile-proprioceptive facilitation. | |||
| Self-care | To increased self-care activities | Activity configurational approach | Multisensory activities |
| Spatial oriental activities | |||
| Achievable activities | |||
| Occupational therapy goal-based activities | |||
| Sensation | To integrative sensation | Multisensory
strategy |
UE-Tactile Kinesthetic activities |
| Vestibular-Proprioceptive activities | |||
| LE-Tactile kinesthetic activities | |||
| Muscle strength | a strength of grade | Biomechanics FOR | ROM-Assistive-maximum to resistive Range of motion |
| Hand function | Hand functional activities | Contemporary Task oriented Therapy | Affected both side-involving activities maximum as per ACA movement therapy protocol activities |
Outcome measure
Table 1: Characteristic of data pre-post-evaluation- Modified Ashworth scale (MAS)
Characteristic of data-Unpaired t-test |
pre-test Intervention (MAS) |
post-test intervention (MAS) |
| Mean | 4.71 | 0.57 |
| standard deviation | 0.49 | 0.53 |
| standard error (SE) means | 0.18 | 0.20 |
| 95% confidence interval difference | 3.31 | 4.97 |
Table 1; data shows (MAS) pre-post-test evaluation scores of all scale components of subject mean values are 4.71and 0.57, respectively standard deviation 0.49 and 0.53 respectively sample size, standard error of mean 0.18 and 0.20, the mean of pre and Post intervention 95% 01confidence interval of this difference 3.31 and 4.97, respectively.
Table 2: The’t test between characteristics of data pre-post-evaluation – Modified Ashworth scale (MAS)
S.No. |
Variable1 |
Variable2 |
Pvalue |
tvalue |
Level ofSignificance |
| 1 | pre-test intervention | post-test intervention | 0.0001 | 12.1824 | statistically Significant |
Graph 1: Mean of Pre control and pre-experimental groups of evaluation -Modified Ashworth scale (MAS)
Table 3: Characteristic of data pre-post-evaluation- wee FIM
Characteristic of data-Unpaired t-test |
pre-test intervention (weeFIM) |
post-test intervention (weeFIM) |
| Mean | 1.00 | 5.72 |
| standard deviation | 0.00 | 0.46 |
| standard error (SE) means | 0.00 | 0.11 |
| 95% confidence interval difference | 4.95 | 4.49 |
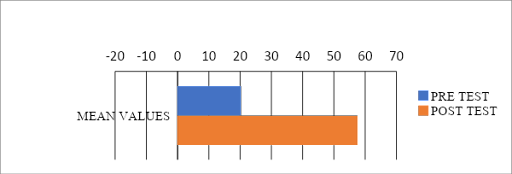
Table 3; Data shows (FIM) pre-post-test evaluation scores of all scale components of subject, mean values are1.00 and 5.72, respectively standard deviation 0.00 and 0.46 respectively sample size, standard error of mean 0.00 and 0.11, the mean of pre and post intervention 95% 01confidence interval of this difference 4.95 and 4.49, respectively.
Table 4: The’t test between characteristics of data pre-post-evaluation- wee FIM
S.No. |
Variable1 |
Variable2 |
Pvalue |
tvalue |
Level ofSignificance |
| 1 | pre-test intervention | post-test intervention | 0.0001 | 43.4697 | Significant |
Graph 2: Mean of characteristics of data pre-post-evaluation-Wee FIM
Table 5: Characteristic of data pre-post-evaluation- Activity based configurational checklist ABCD
Characteristic of data-Unpaired t-test |
pre-test intervention (ABCD) |
post-test intervention n (ABCD) |
| Mean | 42.00 | 12.00 |
| standard deviation | 8.37 | 4.47 |
| standard error (SE) means | 3.74 | 2.00 |
| 95% confidence interval difference | 14.79 | 45.21 |
Table 5; Data shows (ABCD) pre-post-test evaluation scores of all scale components of subject mean values are 42.00 and 12.00, respectively standard deviation 8.37 and 4.47 respectively sample size, standard error of mean 3.74 and 2.00, the mean of pre and post intervention 95% 01confidence interval of this difference 14.79 and 45.21, respectively.
Table 6: The ‘t test between characteristics of data pre-post-evaluation- Activity based configurational checklist- ABCD
S.No. |
Variable1 |
Variable2 |
Pvalue |
tvalue |
Level ofSignificance |
|
| 1 | pre-test Intervention | post-test intervention | 0.0054 | 5.4772 | Very statistically
Significant |
Graph 3: Mean of Pre control and pre-experimental groups of evaluation – Activity based configurational checklist ABCD
Discussion
The purpose of the study is to determine efficacy of early diagnosis and integrated approaches to paediatric occupational therapy on Acute Disseminated Encephalomyelitis. Treatment plan decided was to do Activity Based Configurational checklist- ABCD performance pre and post intervention followed by occupational therapy application, also along with extraction of retained primary self-care management followed by WeeFIM 7-point rating scale.
Data shows (FIM) pre-post-test evaluation scores of all scale components of subject, mean values are1.00 and 5.72, respectively standard deviation 0.00 and 0.46 respectively sample size, standard error of mean 0.00 and 0.11, the mean of pre and post intervention 95% 01confidence interval of this difference 4.95 and 4.49, respectively.
Data shows (MAS) pre-post-test evaluation scores of all scale components of subject mean values are 4.71and 0.57, respectively standard deviation 0.49 and 0.53 respectively sample size, standard error of mean 0.18 and 0.20, the mean of pre and Post intervention 95% 01confidence interval of this difference 3.31 and 4.97, respectively. data shows (ABCD) pre-post-test evaluation scores of all scale components of subject mean values are 42.00 and 12.00, respectively standard deviation 8.37 and 4.47 respectively sample size, standard error of mean 3.74 and 2.00, the mean of pre and post intervention 95% 01confidence interval of this difference 14.79 and 45.21, respectively.
The advantage of combining a developmental approach based paediatric occupational therapy of treatment with the activity configurational approach in the baby own home is that this modification is better accepted by both parents and the baby, as reported by authors such as, who showed better rates of parental competence among those who had applied developmental approach-based treatment.
Conclusion
Efficacy of early diagnosis and integrated approaches of paediatric occupational therapy on Acute Disseminated Encephalomyelitis, with functional ability difficulties is presented. Its role in enhancing participation, and improving functional ability by self-care, facilitation of babys upper and lower extremities performance by activity configurational approach-based therapy described. Day to day function improved satisfactorily. Occupational Therapy focuses on the goal setting and improving childs hand function, thereby enhancing and promoting flexor synergy pattern to extensor synergy pathway (centre of gravity) wise recovery. Occupational Therapy analysis includes an understanding of the internal and external factors and contexts that facilitate independent performance.
Limitations of the study
This case study has several limitations. First, given the broad scope of the study and the amount of literature within each diagnostic category, it was possible to provide only a general synthesis of the overall effect of paediatric occupational therapy intervention strategies. We were not able to include detailed metaphors of case study for direct comparison; however, descriptions of the interventions and characteristics are provided in Supplemental Table 1,2,3,4, for orientation and comparison. We were unable to leach out the effects of variations in activities and specific characteristics of individual ADEM interventions (e.g., type of activities, settings for internal factor affecting modalities). The issue with collection of data on Paediatric Occupational Therapy interventions was frequently noted, indicating a need for more thought in the design of future ADEM rehabilitation future research studies.
References
- Anlar B, Basaran C, Kose G, Guven A, Haspolat S, Yakut A, et al. Acute disseminated Encephalomyelitis in Children: Outcome and Prognosis. Neuropediatrics. 2003; 34:194-9.
- Ascherio A, Munger K. Epidemiology of Multiple Sclerosis.From Risk factors to Prevention. Semin Neurol. 2008; 28:17-28
- Dale RC, de Sousa C, Chong WK, Cox TC, Harding B, Neville BG. Acute disseminated encephalomyelitis, multiphasic disseminated encephalomyelitis and multiple sclerosis in children. Brain. 2000; 123:2407-22.
- Grimsby G, Gudjonsson G, Rodhe M, Sunnerhagen KS, Sundh V, Ostensson ML. The functional independence measure in Sweden:experience for outcome measurement in rehabilitation medicine.Scand J Rehabil Med 1996; 28: 51-62.
- Hamilton B, Granger C, Shervin F, Zielezny F, Tashman J. A uniform national data system for medical rehabilitation. In: Further M, ed. Rehabilitation outcomes: analysis and measurements. Baltimore, MD: Paul H Brooks; 1987, p. 137-147.
- Hynson JL, Kornberg AJ, Coleman LT, Shield L, Harvey AS, Kean MJ. Clinical and neuroradiologic features of acute disseminated encephalomyelitis in children. Neurology. 2001; 56:1308-12.
- Menge T, Hemmer B, Nessler S, Wiendl H, Neuhaus O, Hartung HP, et al. Acute disseminated encephalomyelitis: An update. Arch Neurol. 2005; 62:1673-80.
- Moscovich DG, Singh MB, Eva FJ, Pari BK. Acute disseminated encephalomyelitis presenting as an acute psychotic state. J Nerv Ment Dis 1995; 183: 116-117.
- Panicker JN. Bangalore: National Institute of Mental Health and Neurosciences, NIMHANS (Deemed University); 2004. Acute Disseminated Encephalomyelitis: Clinical Profile and Predictors of Outcome (dissertation)
- Patel SP, Friedman RS. Neuropsychiatric features of acute disseminated encephalomyelitis: a review. J Neuropsychiatry Clin Neurosci 1997; 9: 534-540.
- Tenembaum S, Chamoles N, Fejerman N. Acute disseminated encephalomyelitis: A long-term follow-up study of 84 pediatric patients. Neurology. 2002; 59:1224-31.
- Weir AM, Paton A, Pentland B. Acute disseminated encephalomyelitis: a case history. Eur J Disord Commun 1993; 28: 405-413.
