
Lung disease is the second most common cause of mortality in India following ischaemic heart disease. Representing nearly 20% of the world population, India is shouldering a third of the global burden of respiratory diseases. Patient outcomes in chronic and end-stage lung disease, despite maximal medical therapy is dismal. When referred in a timely fashion to a tertiary advanced lung disease and thoracic transplant centre, a significant number of these patients will benefit from lung transplantation, symptomatically, prognostically, and particularly in respect of quality of life. Although around 5000 lung transplantations are performed globally every year (3), this validated and standard-of-care life-saving procedure is only available in a limited number of countries. It has been available in India for over a decade, but despite many centres having formal authorization, only a limited number of them, less than 10 are active and performing lung transplantation.
There are many systemic, jurisdictional, socioeconomic, cultural, logistical, and clinical reasons why the volume of lung transplantation activity falls so short of the rising national demand. Globally, there is an excess demand for lungs than the available supply of suitable donor organs, leading to prolonged waiting periods resulting in patients either deteriorating further and becoming inoperable, or passing away on the transplant waitlist while waiting for matching donor lungs. Unlike liver and kidney transplants, most lung transplants, barring a small and selective Japanese program, must rely on brain dead or deceased organ donation.
A lung transplant program needs to be delivered by an experienced multi-disciplinary team, rather than simply at the interest of a transplant surgeon or pulmonologist. This, together with requirement for special infrastructure and equipment, has meant that in India almost all active lung transplant centres are based in the corporate sector. Given the delegation of healthcare to individual states in India, there is a significant inter-state variation in the availability and amount of financial support for transplantation. When patients are referred late with onset of significant frailty and additional comorbidities, it becomes almost impossible to deliver the therapy within the allocated and often capped central budget. Whilst early referrals would help immensely towards treating more patients, this needs to be kept in perspective of the underlying culture where the lack of belief in lung transplantation as a viable solution is still prevalent amongst both patients and physicians alike. Despite significant government supported programs to increase public awareness, and modest rises in organ donation in some states, the overall organ donation rate in India remains poor at less than 1 per million population as compared to about 15 to 45 per million population in developed countries.
Similarly, logistical issues also impact significantly on donor lung utilization. Donor assessment and multi-organ retrieval from a deceased donor typically occurs overnight or in the early hours of the morning. When the donor is in a rural setting, or even in a second tier cities, there can be major out-of-hours issues with both air and road travel in keeping the cold ischemic time of the organ within a safe time limit, with the consequence that even good organs may go wasted. Where this can be mitigated by private air charter, the financial burden is beyond consideration for most Indian recipients. These combined factors are responsible for excluding the majority of donor lungs for transplantation. The most significant steps in improving donor organ utilization would be that of standardising donor management to long-established multi-organ donor protocols, and a greater flexibility in the time available for the retrieval teams to assess, and if need be, to implement strategies for improving organ function to an acceptable state.
The current practice utilises cadaveric organs from donation after brain death (DBD). The other pathway is that of organ donation following circulatory death (DCD). The outcomes from utilisation of DCD donor lungs is excellent and non-inferior to the general use of DBD lungs. In January 2023, a five-judge constitution bench at the Indian Supreme Court strengthened its Article 21 in advancing the right to die with dignity, and modified the previous 2018 Euthanasia Guidelines. It was decreed that withdrawal of life-support, or passive euthanasia, could be carried out to alleviate the suffering of terminally ill patients who are unable to communicate their wishes. The ruling applies to both situations where there is a patient-directed Advanced Medical Directive in place, and also when it is absent, in which scenario, the patient’s family and advocates take on this responsibility while assisted by the clinical team. This new ruling permits the withdrawal of life support within its definition and therefore opens a welcome opportunity to further expand the deceased donor pool for the benefit of dying patients on transplant waitlists. On the background of sociocultural hurdles, as well as those related to a wider public and professional acceptance of lung transplantation, it will necessitate a courageous State and its transplant regulatory authority to permit piloting a DCD program for solid organ transplantation.
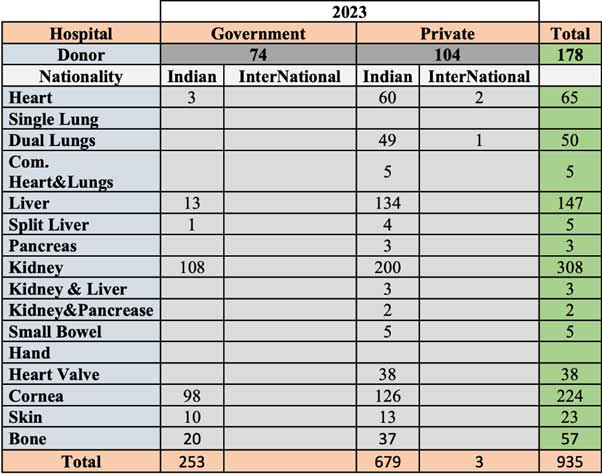
Table 1 below, shows data from the Transplant Authority of Tamil Nadu (TRANSTAN) which clearly elaborates on the poor utilization of lungs in the state of Tamil Nadu. In the year 2023, out of a total of 178 donations in the state of Tamil Nadu, 50 lungs were utilized. Given that this number counts each lung rather than each pair, the actual for number of double lungs utilized for transplants in 2023 were 25. There were no single lung transplants that year. The lung utilization rate is therefore poor at only 14%.
The only other way to improve the function of suboptimal donor lungs, is an expensive strategy requiring organ perfusion. There are currently only two devices approved by the FDA (USA) for commercial use in lung transplantation. The first is the Transmedics OCS Lung System which permits the donor lungs to be implanted on a normothermic perfusion circuit allowing the lungs to be ventilated and assessed during the transportation back to the transplant centre and thereafter. The second is the XVIVO Perfusion System which involves bringing the retrieved lungs back to the transplant centre under standard static cold storage preservation, and then implanting the organs on to the XVIVO perfusion device. Both devices are useful in reconditioning donor lungs that are oedematous and when there is insufficient time to reverse the pulmonary oedema in the donor prior to organ retrieval. In either scenario, the successful reconditioning of the donor lung for conversion to a transplant cannot be guaranteed and the question of who then pays for the failed resuscitation is a major hurdle. The current costs of these devices make their adoption unaffordable in the Indian context. Local development of such technology, with local manufacture, and at locally affordable prices would make a significant positive impact on donor organ utilisation. The fact is that the real role for these devices is not in merely drying out oedematous lungs, but their value as ex-situ platforms for a host of other therapeutic purposes. These include, pharmacological interventions such as high dose antibiotics for underlying pneumonia without having to worry about systemic effects, genomic and proteomic therapies to attenuate the expression of pro-inflammatory genes, and use of immune modulation and stem cell therapies, all focused on improving donor lung function with mitigation of ischaemi-reperfusion-injury, reduction of primary graft dysfunction, and importantly as a comprehensive strategy towards influencing a reduction in chronic lung allograft disease in the medium term. Remarkably, the platform has also been successfully used to convert type A donor lungs into type O universal donor type lungs.
The Way Forward:
- Donor Management
State transplant authorities need resources to maintain sufficient donor coordinators who oversight donor management, provide dispassionate communication, and are tasked to maximize the opportunity for multi-organ donation and subsequent conversion to clinical transplants. - State run air ambulances
With inter-state integration, this would provide a cheaper alternative to nationally increase the availability of distantly located organs for Indian recipients. - Organ Perfusion Technology
Consider funding the local development and manufacture of affordable lung perfusion devices, as is happening for renal and hepatic organs. - Utilization of lungs from Donation after Circulatory Death (DCD)
References
-
- https://www.worldlifeexpectancy.com/country-health-profile/india
- Prasad KT, Sehgal IS, Dhooria S et al. Patient characteristics and outcome of end-stage lung diseases referred for lung transplantation in North India. Lung India. 2018;35(4):290-294
- Chambers DC, Perch M, Zuckermann A et al. The International Thoracic Organ Transplant Registry of the International Society for Heart and Lung Transplantation: Thirty-eighth adult lung transplantation report – 2021; Focus on recipient characteristics. J Heart Lung Transplant. 2021;40(10):1060-1072
- van der Mark SC, Hoek RAS, Hellemons ME. Developments in lung transplantation over the past decade. Eur Respir Rev. 2020;29:190132
- International Registry in Organ Donation and Transplantation. Preliminary Numbers. 2017. Available from: http://www.irodat.org/img/database/pdf/NEWSLETTER2018_June.pdf
- Organ Procurement and Transplantation Network. Donor Type by Organ Type and Transplant Year. https://optn.transplant.hrsa.gov/data/
- dos Santos PAR, Teixeira PJZ, de Moraes Dm et al. Donation after circulatory death and lung transplantation. J Bras Pneumol 2022; 48(2):e20210369
- Transtan Year Book 2023. https://transtan.tn.gov.in/statistics-new.php
- Halpern S, Kesseli S, Au S et al. Lung transplantation after ex vivo lung perfusion versus static cold storage: An institutional cost analysis. Am J Transplant 2022;22:552-564
- Prasad N, Pasrija C, Talaie T et al. Ex vivo lung perfusion: Current achievements and future directions. Transplantation 2021; 105(5):979-985
- Wang A, Ribiero RVP, Ali A et al. Ex vivo enzymatic treatment converts blood type A donor lungs into universal blood type lungs. Sci Transl Med 2022; 14(632):eabm7190

Dr. Ram Duvuru
Senior Consultant – Cardiac Transplant Surgery

Dr. Prakash M Ludhani
Senior Consultant – Cardiothoracic & Vascular Surgery (CVTS), Heart & Lung Transplantation and MCS

Dr. Pradeep Kumar
Director – Transplant Pulmonology and Lung Failure Unit

Dr. Srinivas Rajagopala
Director – Interventional Pulmonology and Sleep Medicine
Director – Transplant Pulmonology and Lung Failure Unit
Dr. Kumud Kumar Dhital
Program Director – Heart and Lung Transplantation
Department of Heart & Lung Transplantation & Mechanical Circulatory Support
Kauvery Hospital, Vadapalani, Chennai
