A case report on severe dental caries with advanced lesions
Esther Jayamary1, Cecily Ruba2, Mahalakshmi3
1Nursing Supervisor, Kauvery Hospital, Cantonment
2Nurse Educator Kauvery Hospital, Cantonment
3Nursing Superintendent, Kauvery Hospital, Cantonment
Abstract
Dental caries is a bio film-mediated, sugar-driven, multifactorial, dynamic disease that results in the phasic demineralization and remineralization of dental hard tissues. Caries can occur throughout life, both in primary and permanent dentition, and can damage the tooth crown and, in later life, exposed root surfaces. The balance between pathological and protective factors influences the initiation and progression of caries. This interplay between factors underpins the classification of individuals and groups into caries risk categories, allowing an increasingly tailored approach to care. Dental caries is an unevenly distributed, preventable disease with considerable economic and quality-of-life burdens. The daily use of fluoride toothpaste is seen as the main reason for the overall decline of caries worldwide over recent decades. This Primer aims to provide a global overview of caries, acknowledging the historical era dominated by restoration of tooth decay by surgical means, but focuses on current, progressive and more holistic long-term, patient-centred, tooth-preserving preventive care.
Background
The process of dental caries is multifactorial, involving the interaction of three key elements: susceptible tooth surfaces, dietary sugars, and the presence of cariogenic bacteria in the mouth. These bacteria, primarily Streptococcus mutans and Lactobacillus species, metabolize sugars from food and produce acids as a byproduct. This acidic environment erodes the enamel and, if not neutralized, continues to affect deeper layers of the tooth, such as dentin.
The disease typically progresses in stages:
- Demineralization: The initial phase is marked by the loss of minerals from the tooth surface due to the acid attack. This leads to the formation of white spots on the enamel.
- Cavity formation: If the process continues, the enamel becomes compromised, and the soft tissue beneath (dentin) is exposed. At this point, a visible hole or cavity forms.
- Advanced decay: If left untreated, the decay can progress deeper into the tooth, affecting the pulp, which contains nerves and blood vessels. This can lead to pain, abscess formation, and eventual tooth loss.
Case Presentation
32 years aged female patient was admitted with complaints of decayed teeth in the upper and lower jaw. She has been bedridden for the past 3 yrs because she had non-hemorrhagic stroke that was treated abroad. Patient was on prolonged invasive ventilation and Tracheostomy, weaning was done gradually, and rehabilitation was given over 6 months. The tracheostomy was closed. Oral feed was started. Patient was unable to swallow food, she always kept the food in her mouth for a long time hence she developed tooth caries.
Social history
She did not have history of cigarette smoking or alcohol addiction.
Allergic History
No known medicine or environmental allergy.
Past Medical History
No known medical history
Past Surgical History
LSCS on 2022
Physical examination
RR: 20/min, Blood Pressure: 120/80mm Hg, Temperature: 90.8°F
Physical examination of teeth
Overall Appearance: Mild discoloration over the lower molars, tooth cavity present.
Tooth Surface: signs of demineralization present and advanced tooth decay present in the molar 15, 14, 13, 12, 11, 21, 22, 23, 24, 25, 26, 35, 34, 33, 32, 31, 41) including pulp and Extensive deacy in extensive decay in 13, 12, 11, 21, 22,23.
With moderate to severe caries lesions in the 18, 17, 16, 27, 28, 35, 36, 37, 38, 46, 47, 48 molar
Plaque and Tartar: The presence of plaque or tartar buildup was noted, on the mandibular incisors.
Alignment and Positioning: Each tooth was straight with no crowding or no spacing.
General Examination
Patient was conscious/fair/aphasic/not obeying commands
GCS 13/15
Initial Evaluation
| S. No | Investigations | Results |
|---|---|---|
| 1 | Hb | 13.4 |
| 2 | PCV | 40.4 |
| 3 | WBC | 7300 |
| 4 | TSH | 6.17 |
| 5 | Free T4 | 1.04 |
| 6 | PT | 12.5 |
| 7 | Control | 11.5 |
| 8 | HIV | Negative |
| 9 | HbsAg | Negative |
| 10 | Antibody | Negative |
Treatment
Procedure Summary
The patient was prepared and draped following all standard sterile precautions. Under general anesthesia (ET GA), the following procedures were performed:
Root Canal Treatment (RCT) was completed on the following teeth: 15, 14, 13, 12, 11, 21, 22, 23, 24, 25, 26, 35, 34, 33, 32, 31, and 41.
The procedure was carried out with 2% Lidocaine (LA) infiltration for local anesthesia.
Glass Ionomer Cement (GIC) Entrance Filling was placed to seal the access cavities.
Light-Cured (LC) Fillings were applied in the following teeth: 13, 12, 11, 21, 22, and 23.
GIC Restorations were placed in the following teeth: 18, 17, 16, 27, 28, 35, 36, 37, 38, 46, 47, and 48.
The procedure was completed without complications. The patient’s recovery was normal and uneventful.
Management
Patient was initially treated with Tab. Aceclofenac CR P –SOS, Tab. Paracetamol 500mg SOS
Follow up also advised with Analgesics.
Review advised after a week.
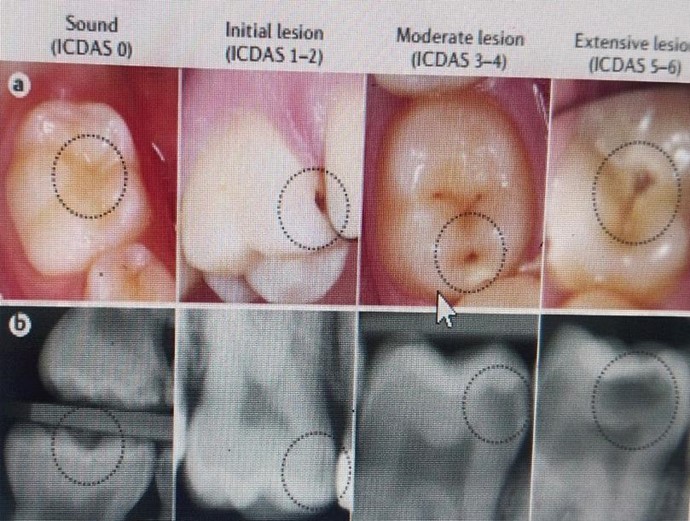
Clinical and Radiographic appearance of the stages of severity of tooth decay
Nursing Management
1. Assessment
- Pain and Comfort: Since the patient was aphasic, assessing pain through non-verbal cues was crucial. Looked for signs such as facial grimacing, restlessness, or changes in vital signs that could indicate discomfort.
- Oral and General Health: Assessed the patient’s oral cavity regularly to check for signs of infection, bleeding, or complications from the extraction. Monitored the overall condition, including their ability to tolerate food and fluids, as well as their general well-being.
2. Pain Management
- Non-Verbal Pain Assessment: Since the patient could not verbalize pain, behavioral indicators were used such as restlessness, changes in facial expression, and guarding of the mouth. Utilized pain assessment tools designed for non-verbal patients.
- Pain Relief Administration: Administered pain medications as prescribed. For a bedridden patient, opt for liquid analgesics or crushed medications, if necessary, to ensure proper dosing.
- Cold Compress: Applied a cold compress to the face in 15-minute intervals to help reduce swelling and pain, ensuring the patient’s comfort.
3. Preventing Infection
- Post-Extraction Care: Instructions given to the caregivers or family members on the importance of keeping the extraction site clean to avoid infection. Since the patient was bedridden, it was challenging for her to perform oral hygiene independently, so assistance with oral care was necessary.
- Oral Hygiene Assistance: Since the patient was unable to perform oral care due to aphasia, instructions were given to the caregiver to gently clean the oral cavity. Used a soft toothbrush or a gauze pad with a mouthwash (like saline or chlorhexidine) to wipe the inside of the mouth. Avoided disturbing the extraction site.
4. Wound Healing
- Monitor for Complications: Instructed to check the extraction site regularly for signs of complications, such as excessive bleeding or dry socket, especially as the patient had limited mobility, which may impact blood flow to the area.
- Diet Modifications: Since the patient was bedridden, advised to ensure that she received a soft, nutritious diet. Offered foods that were easy to swallow and that won’t irritate the extraction site. Liquids were offered in a form that the patient could manage, with a syringe or special cup when swallowing was an issue.
- Hydration: Advised to Ensure the patient was adequately hydrated, as dehydration can slow the healing process. Hydration was encouraged, with careful attention to the patient’s swallowing ability.
5. Managing Communication Barriers (Aphasia)
- Communication Techniques: Since the patient was aphasic, used alternative communication methods to understand her needs. This involved using gestures, facial expressions, or picture boards, or relying on family members or caregivers who knew how to communicate with the patient.
- Provide Reassurance: Offered reassurance with non-verbal cues (like a calm voice, touch, and facial expressions) to help reduce any anxiety or frustration the patient may experience due to their inability to speak.
- Involve Family Members: Involved family members or caregivers in the care process. They can help communicate the patient’s needs, assist with oral care, and provide emotional support during recovery.
6. Managing Potential Complications
- Monitor for Dry Socket: Watched for signs of dry socket, which can occur if the blood clot had dislodged. Symptoms include severe pain in the extraction site, which may radiate to the ear. The patient might be unable to express this pain, so watched for restlessness or grimacing.
7. Patient and Caregiver Education
Post-Extraction Instructions: Since the patient iwas aphasic, educated the family and caregivers . Provided clear written or verbal instructions about post-operative care, including:
- The need to monitor for infection or complications.
- How to assist with oral hygiene.
- How to administer medications, if applicable.
- What to do if excessive pain, swelling, or bleeding occurs.
Dietary Recommendations: Emphasized a soft-food diet to avoid irritation to the extraction site and to facilitate swallowing for the bedridden patient.
8. Follow-Up Care
- Post-Op Visit Preparation: Arranged for a caregiver or family member to accompany the patient to follow-up appointments, ensuring they can communicate the patient’s needs and provide necessary support.
- Advised for proper follow up.
Conclusion
In conclusion, the management of severe dental caries with advanced lesions in a bedridden patient with a tracheostomy presented unique challenges. The patient’s condition required careful attention to pain management, infection prevention, and postoperative care, particularly following a surgical treatment like Root Canal Therapy (RCT) with Glass Ionomer Cement (GIC) for restoration. Effective nursing care and support were critical to ensuring the patient’s comfort, especially in the context of communication barriers and the need for assisted oral hygiene. Postoperative monitoring was essential to detect potential complications such as infection or improper healing. Education for caregivers on proper oral care and diet was crucial in preventing future caries. Multidisciplinary collaboration, including coordination with physical therapists and speech therapists, enhanced recovery and supported the patient’s overall well-being. Regular follow-up was advised to ensure long-term oral health. In sum, holistic care tailored to the patient’s specific needs was the key to her successful recovery and quality of life post-surgery.
Ms. Esther Jayamary
Nursing Supervisor
Ms. Cecily Ruba,
Nurse Educator
Mahalakshmi
Nursing Superintendent
