Having doctors at home definitely had an impact on Dr Mahalakshmi to choose Medicine as her profession.
How did she choose Anesthesia as her speciality? This credit goes to her friends Anitha and Preethi who were the sole reasons for her choice.
It suited her personality of multi tasking, and she felt it gave her a great work life balance.
It has been a roller coaster ride with full of adrenaline rush. She’s proud of her choice of Anesthesia as her specialty.
She says it’s a unique field though there is not much awareness regarding what an Anesthetist does.
Dr Mahalaksmi works to create on the impact and importance of Anesthetists by writing for K-Way.
She believes in keeping an active healthy lifestyle by indulging in any physical fitness form like dance or yoga.
Also learning various skills like swimming, silambam, skating and trekking. She feels learning has no limits and age is just a number.
Time is very valuable and should be spent wisely to improve physical and mental health.
This procedure of venepuncture to get access to a vein is a common procedure experienced by many patients. Though it may look like an easy task, it requires considerable practice to be perfect. The venflon prick frightens almost all patients irrespective of their age. However, venous access is mandatory for all the in-hospital patients and for patients planning for (or undergoing) procedures.

What Is an IV Cannula?
It is a small plastic tube inserted into a vein. Veins carry blood from all parts of your body to your heart; only veins give direct access to administer drugs and fluids.
The main purpose of an IV cannula – fluid therapy, drug administration, chemotherapy, blood transfusion, and nutrition in long-term hospitalization and intra-venous sedation and for patients undergoing procedures (endoscopy, bronchoscopy, colonoscopy, chemotherapy, lumbar puncture, epidural steroid, dialysis catheter insertion), angiogram procedures and surgeries all need intra venous access.

If a patient is undergoing imaging i.e., MRI, CT, angiograms with contrast, he/she needs intravenous access for contrast dye injection.
So, How Is It Secured?
We always make sure that the patients are in a comfortable position, mostly secured in their hands i.e., left hand, hence it helps them to have their dominant hand free for movements; the side is chosen according to the site of the procedure or surgery. The size of the cannula is chosen depending upon the type of surgery, positioning of the patient during surgery, need of drugs, blood transfusion, higher antibiotics, etc.
An IV cannula is secured at the time of admission if the patient is in need of fluid therapy, intravenous drug therapy and antibiotics, or else 2 hours before the procedure for hydration depending upon the fasting status of the patient.
How Do We Secure in Paediatric Age Group?

We apply local anaesthetic cream 30-45 minutes before in the areas where the veins are visible. If the child is cooperative, we secure the IV with the help of parents or a nurse by their bedside.
In case of anxious children posted for surgeries, we shift them to the theatre and make them inhale anaesthetic gases which put them to sleep and then secure the IV. We also give them oral sedative syrup or intramuscular injection of a sedative (inj. Ketamine) to keep them calm in the preoperative holding area. Once they fall asleep, IV can be secured. This also applies to patients undergoing procedures outside the operating room as well as to adults who are anxious and not willing to get the needle prick when they are conscious.
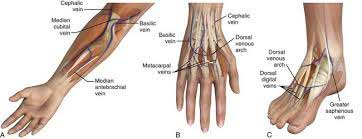
The sites of peripheral IV cannulation are most commonly in hands – forearm and cubital. The foot is used as a site only when access to the hand is not possible. For example, in burns, AV fistula, hand surgeries, a patient who has undergone lymph node dissection, etc.
An external jugular vein in the neck is cannulated when hands and legs access is not a choice, also in cases where there is a need for wide bore cannula for higher concentrated drugs.
Indication for Central Line
The jugular vein and femoral vein are cannulated for high-risk surgeries, critically ill patients, parenteral nutrition, for those who require blood sampling often, prolonged hospitalization, major burns and poor peripheral IV access.
For How Long Can an IV Cannula Be Retained?
3 days maximum. All the IV lines carry a plaster mentioning the date and time it was secured. An IV line is secured under sterile precautions and flushed to make sure of free flow and patency before dressing. Patients are reassured if they are anxious about the pain of the cannula. A recheck for blockage is done if there is no free flow. In our hospital, we have a separate team that inspects the IV cannula to avoid cannula-related infection and complications.
Extravasation
This is the infiltration of a drug from an IV line into the surrounding tissue. This will cause pain, swelling and coolness of the skin around IV cannula.
Occlusion
Slowing or cessation of fluid infusion happens when IV is disconnected and reconnected after a gap. At times, a flush to unblock the clot will help to clear out the blockage.
Thrombophlebitis

Inflammation of a vein. Tenderness, and redness will be present.
When there is redness, swelling and pain, leaking from cannula, thickening of the vein like a cord at the site of the intravenous cannula, the cannula will be removed immediately.
Dos and Don’ts
A patient can be mobilized and can carry out the routine activity with an IV cannula. They can cover up the area with a glove or plastic cover when in need of restroom breaks. The IV site should not be wet. Most importantly, the IV site should be kept clean and visible.
Recently, we had two patients who had a history of difficult IV access and they were extremely worried about how their IV will be secured. One gave history of syncopal attack while she had her IV secured during her previous admission elsewhere. The other patient had a history of 30 pricks for IV cannula before her surgery in the past. In the preanesthetic clinic assessment, they requested that they should not go through the trauma again for an intravenous line. It was a challenging task, as their veins were hardly visible. Firstly, 45 minutes prior, the local anaesthesia cream was applied over the hands, cubital and forearm. Furthermore, the previous night, both these patients were given a small dose of anti-anxiety medication to make sure they got a sound sleep. Secondly, they were given inhalational anaesthetic agents and put to deep sleep and then IV was secured. Most importantly, all these plans were clearly informed to the patient & family; they were reassured that they will receive the utmost care and they will not feel pain at all.
For Whom Are the Veins Difficult to Cannulate?
Obese, low platelet count, severe dehydration, thin and tortuous course of veins, bleeding disorders, post chemo and radiotherapy.
To make the veins more visible, we ask the patients to open and close their hands by making a fist for 5-10 times. This improves blood flow through the veins and helps in visibility. Tourniquet – a tight band is tied to gadgets of recent advanced science that eases such difficulties. Ultrasound, vein markers make it easier for both patients & doctors.
Tips to Keep Our Veins Healthy
Hydration helps the veins to have a good amount of blood flow and makes the veins visible. Active lifestyle – walking, and movement of the body makes the blood circulation active.

Dr. K. Mahalakshmi
Consultant Anaesthesiologist
Kauvery Hospital Chennai
