A case study on hydatid cyst
Harini R
PharmD Intern, Kauvery Hospitals, Trichy
Correspondence: harinir636@gmail.com
Abstract
A 66-year-old male presented with abdominal pain and swelling. Further investigations showed a Hydatid Cyst in the liver. He underwent surgery where the cyst was removed. Post-operative period had complications that were treated. He recovered soon.
Case Presentation
A 66-year-old male presented with swelling in the upper abdomen for three years in outpatient department with chief complaints of abdomen pain, vomiting (1 episode), loss of appetite, weight loss and a very yellow coloured urine.
Social History: Smoker; he smoked 1 pack of cigarettes per day for 30 years and consumed alcohol for 30 years (3/7) 1 quarter.
Allergies: No known medicine, food, or environmental allergies.
Past Medical History: Hypertension, Cerebral vascular accident.
Past Medication History: He was irregular on taking medicines.
Past Surgical History: Not known history.
Physical Examinations
Vitals: Temperature: 97.8 F, Heart rate: 78, Respiratory rate: 22, Blood pressure: 130/ 90.
CVS: S1S2(+), RS: BAE (+)
P/A: Soft, irregular swelling x 15 x 20 cm occupying epigastrium, left hypochondrium, cystic ,consistency, moves with respiration
P/R: NAD.
Initial Evaluation
Laboratory Studies: Potassium: 128.4, Sodium: 4.73.
USG abdomen: It showed a liver lesion – a huge hydatid cyst in the liver extending through diaphragm.
MULTISLICE CT-ABDOMEN AND PELVIA- REPORT Non visualization of left lobe of liver. Minimal ascites. Collapse- consolidation of bilateral lower lobes. Extensive subcutaneous emphysema with loculated fluid collection in the anterior abdominal wall, with no intra-abdominal communication. Prostatomegaly.
Diagnosis: Hydatid Cyst
Management And Outcomes
Patient was reviewed in OPD, completed course of Albendazole and was admitted for elective surgery. He had received Albendazole for 3 weeks, Surgical management – left hemi hepatectomy + laparotomy + thoracotomy + cholecystectomy + diaphragmatic repair- was planned and done, later patient was shifted to ICU for further management. Patient was treated with IV antibiotics, IV fluids and other supportive medications. Patient developed oliguria for which a Nephrology opinion was sought and advised hemodialysis. Patient underwent 2 cycles of SLED. There was also a drop in Hb and platelets for which Hematology opinion was sought, orders were carried out. The patient developed hypotension for which inotropes were started and weaned off. The patient received blood transfusion and improved symptomatically. Serial RFT values were on an improving trend and later he was shifted to ward. Patient also received albumin, and NAC infusion. Patient was started on oral diet, tolerated well and opened his bowel. ICD was clamped and removed after verifying adequate lung expansion. Patient had serous discharge from wound site. CT abdomen was done. Bedside wound drainage of abdominal wall and dressed was done in a sterile manner then the patient improved symptomatically and was discharged with the following advice.
Discharge Medications
| S.No | Drug Name | Strength | Frequency | Route of admin | Relationship with meal | Days | ||
| M | A | N | ||||||
| 1 | TAB.OFLIN | 200MG | 1 | 0 | 1 | ORAL | AFTER FOOD | 2 DAYS |
| 2 | TAB.URSOCOL | 150MG | 1 | 0 | 1 | ORAL | AFTER FOOD | 7 DAYS |
| 3 | TAB.TRAMADOL | 50MG | 1 | 1 | 1 | ORAL | AFTER FOOD | 5 DAYS |
| 4 | TAB.PANTOCID | 40MG | 1 | 1 | 1 | ORAL | BEFROE FOOD | 7 DAYS |
| 5 | TAB.ALBENDAZOLE | 400MG | 1 | 0 | 1 | ORAL | AFTER FOOD | 7 DAYS |
| 6 | SYP.CREMAFFIN PLUS | 10ML | 0 | 0 | 1 | ORAL | AFTER FOOD | 7 DAYS |
| 7 | TAB.ALDACTONE | 50MG | 1 | 0 | 0 | ORAL | AFTER FOOD | 1 WEEK |
| 8 | TAB.LASIX | 40MG | 1 | 0 | 0 | ORAL | AFTER FOOD | 1 WEEK |
| 9 | ALBUZEST RENO POWDER | 1 | 0 | 1 | ORAL | AFTER FOOD | 1 WEEK |
Discussion
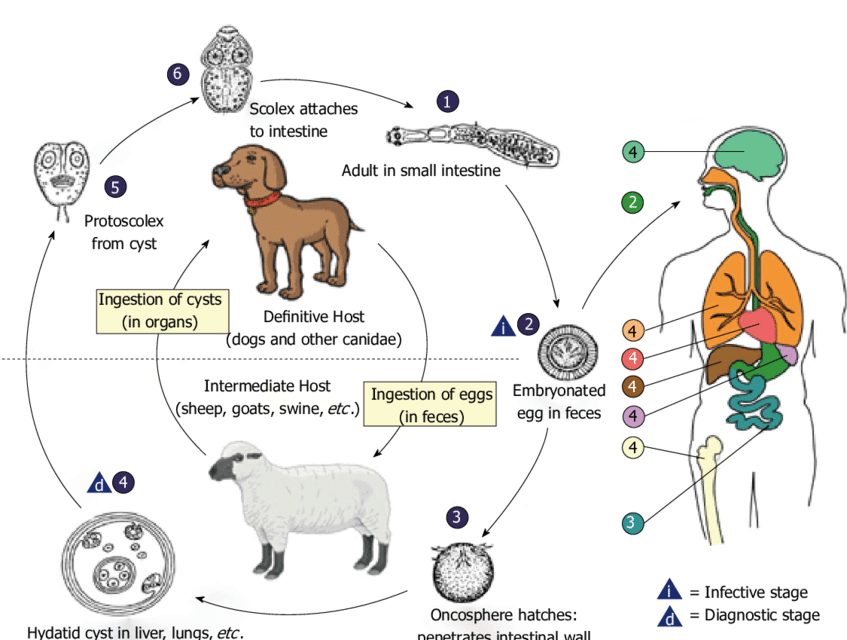
Hydatid cyst is a fluid-filled sac with daughter cysts, usually found in the liver. It is caused by the larval form of the parasite Echinococcus granulosus [1]. Hydatid cysts commonly affect the liver (50-70%) or lung (20-30%), but they can also affect other organs, including the brain, heart, and bones (10%) [2]. The hermaphrodite flatworm E. granuloses has three developmental phases. The pericyst, which is composed of inflammatory tissue from the host, the exocyst, and the endocyst, which produces scoleces (Scolex is singular), and the proligere membrane, make up the cyst’s typical structure [3]. The clinical presentation of hydatid cysts is pain in the abdomen, loss of weight and appetite, abdominal discomfort, and vomiting [4]. With the use of case history and imaging methods like CT scan or MRI, the diagnosis can be made most quickly, even by using ultrasonography. Additionally, serology tests like ELISA and immunoblotting can be employed; however, these tests are only 50-56% sensitive for the lungs and other organs. [5]
The complication of intrabiliary rupture is a frequent occurrence. Other, less frequent problems include the cyst rupturing into the peritoneal cavity, the chest cavity way of the diaphragm and towards the gastrointestinal tract organs, and the cyst developing a secondary bacterial infection [6]. Pharmacological treatment, percutaneous drainage, or surgery (using a traditional or laparoscopic method) are all options for treating Hydatid cysts of the liver. Complex or widespread injuries, older patients, pregnancy, concomitant conditions, numerous cysts that are difficult to access, partially resting or calcified liver cysts, or patient refusal of operation are all reasons why surgery is not advised. In addition to surgical interventions Albendazole therapy is safe and effective for the treatment of hepatic hydatid cysts.
Pharmacological Treatment
Class: Benzimidazoles are indicated for echinococcus
Mebendazole was initially used to treat hydatid cysts. Albendazole, which was more easily absorbed, quickly took the place of the former drug that had poor stomach absorption. The metabolite in Albendazole, Sulfoxide, can diffuse rapidly from the cyst membrane and concentrate in the cyst fluid, giving it better efficacy [8]. Another drug, Praziquantel, is used with Albendazole, combined for more efficacy [9].
Dose
Albendazole: 10 mg/kg/day for 4 weeks
Mebendazole: 40-50 mg/kg in 3 divided doses
Praziquantel: 40-60 mg/kg/day in divided doses.
Mechanism of action
It blocks the glucose uptake in the parasite and glycogen storage by binding with the tubulin [10].
Role of Albendazole
Albendazole treatment before and after surgery declines the ability of the cysts to survive after the surgery and greatly minimizes the possibility of recurrence of cysts [10].
References
- Lasya T, et al. Hydatid cyst: Anywhere, everywhere. Radiol Case Rep. 2011;6(3):486.
- Sabouni F, et al. Multiple Organ Involvement with Hydatid Cysts. Iran J Parasitol. 2010;5(2):65-70.
- Botezatu C, et al. Hepatic hydatid cyst – diagnose and treatment algorithm. J Med Life. 2018;11(3):203-209.
- https://www.cdc.gov/parasites/echinococcosis/disease.html
- Derbel F, et al. Hydatid Cysts of the Liver – Diagnosis, Complications and Treatment [Internet]. Abdominal Surgery. InTech; 2012.
- Alexiou K, et al. Complications of Hydatid Cysts of the Liver: Spiral Computed Tomography Findings. Gastroenterology Res. 2012;5(4):139-143.
- Gavara C, et al. Review of the treatment of liver hydatid cysts. World J Gastroenterol. 2015;21(1):124-31.
- Dehkordi AB, et al. Albendazole and treatment of hydatid cyst, review of literature. Infectious Disorders. 2019;19(2):101-4.
- lvela-Suárez L, et al. Safety of the combined use of praziquantel and albendazole in the treatment of human hydatid disease. Am J Trop Med Hyg. 2014;90(5):819-22.
- Shams-Ul-Bari, et al. Role of albendazole in the management of hydatid cyst liver. Saudi J Gastroenterol. 2011;17(5):343-7.

Ms. Harini R
PharmD Intern
