Benign Paroxysmal Positional Vertigo (BPPV): A Case Series
G.K Balasubramani*,
Senior Physiotherapist, Kauvery Hospital, Salem
*Correspondence: gkbalasubramani027@gmail.com
Introduction
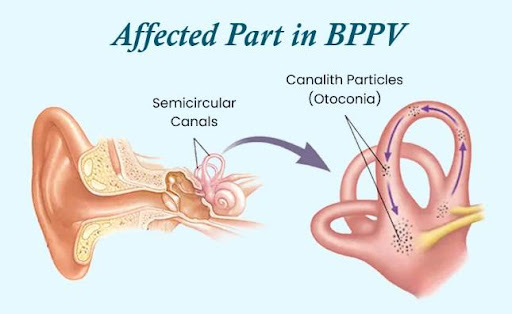
Benign paroxysmal positional vertigo (BPPV) is the most common cause of vertigo arising from peripheral vestibular disorders. It is a condition that causes a sudden onset of vertigo when the head is moved into certain positions. Vertigo is felt as dizziness and is often combined with nausea and nystagmus. BPPV is caused by the dislodging of tiny crystals within the inner ear. The inner ear contains three semicircular canals, which are responsible for telling us whether we are still or moving. Crystals found within these canals stimulate the nerves that sense head movement and, if dislodged, can cause the feeling of dizziness.
Pathogenesis
The Otoconia the calcium carbonate that is present in the macule enters the semicircular canal, and as it travels through the semicircular canal, it induces vertigo and other symptoms such as nausea, vomiting, and nystagmus.
Dizziness and vertigo are among the most prevalent complaints in people of all ages but are common in middle-aged and elderly people and have a major negative influence on (i) the perception of quality of life and (ii) the risk of falling. (iii) affects basic and instrumental activities of daily living. Due to population ageing, particularly in wealthy nations, vertigo represents a growing issue and a serious public health concern. In order to approach the patient safety strategy as well as identify the best repositioning maneuver options according to the clinical scenario of different age populations.
Case Presentation
Case 1
A 48-year-old female presented with a sense of spinning while moving from a standing to sitting position and had a symptom of nausea. There were two episodes lasting a few minutes, and it worsened in the right lateral position. No h/o: diplopia, weakness, headache, dysarthria, hearing loss, tinnitus, allergies there is no history of similar illnesses in the past or in the family.
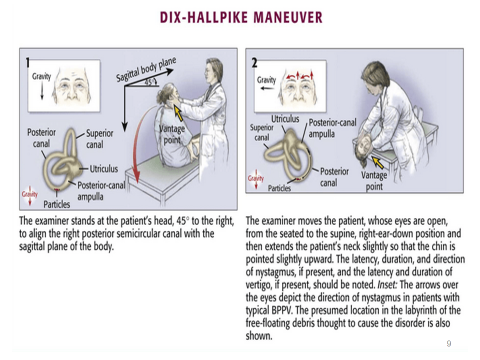
On Examination: conscious, obeying commands, vitals stable. CNS: higher mental functions are normal. Cranial Nerve: Normal Tone- Normal. Muscle power: normal. Romberg signs: postural instability (+) on the right side. Special test: Dix Hall pike test: counter-clockwise nystagmus (+) on the right side. Supine roll test (-). Motion sensitivity quotient: 11-30 sec (moderate). Final
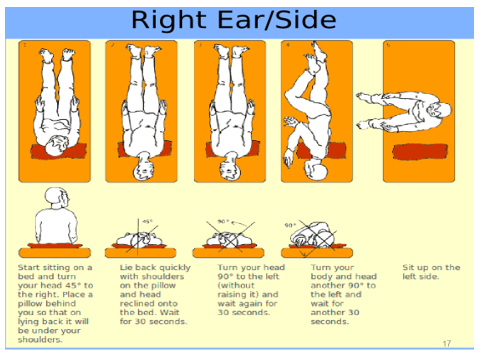
Diagnosis: Right posterior-Semicircular canal BPPV Intervention of the right-sided Epley maneuver, balance, and gaze stability exercises were performed three times per day.
Case 2
A 27-year-old male presented with a sense of dizziness while changing positions from sitting to bending forward to pick something up. There was one episode lasting a few minutes, and it worsened in either side position. No h/o: diplopia, weakness, headache, dysarthria, hearing loss, tinnitus, allergies there is no history of similar illnesses in the past or in the family.
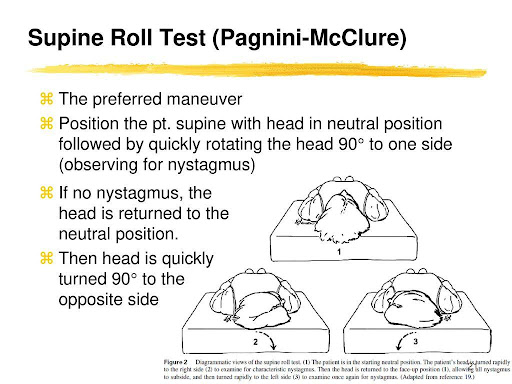
On examination: conscious, obeying commands, vitals stable. CNS: higher mental functions are normal. Cranial Nerve: Normal Tone: Normal Muscle power: normal. Romberg signs: postural instability (+) on both sides Special test: Dix Hall pike test: (-) on both sides. Supine roll test: Horizontal nystagmus (+). Motion sensitivity quotient: 11-30 sec (moderate).
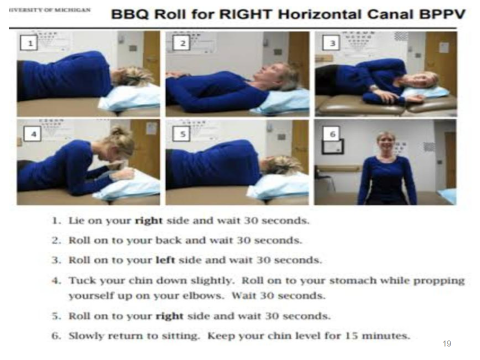
Final Diagnosis: Horizontal-Semicircular canal BPPV Interventions of the barbecue maneuver, balance, and gaze stability exercises were performed three times per day.
Case 3
A 57-year-old male presented with a sense of spinning while getting up from the bed, associated with vomiting and a recent history of viral fever. There were two episodes lasting a few minutes, and it worsened in the right and left side positions. No h/o: diplopia, weakness, headache, dysarthria, hearing loss, tinnitus, allergies there is no history of similar illnesses in the past or in the family.
Examination: conscious, obeying commands, vitals stable. CNS: higher mental functions are normal. Cranial Nerve: Normal Tone: Normal Muscle power: normal. Romberg signs: postural instability (+) on both sides Special test: Dix Hall pike test: (-) on both sides. Supine roll test: horizontal nystagmus (+). Motion sensitivity quotient: above 30 seconds (severe).
Final Diagnosis: Vestibular Neuritis Interventions of the barbecue maneuver, balance, and gaze stability exercises were performed three times per day.
Case 4
A 67-year-old male presented with a sense of dizziness and vomiting while driving a car. There were two episodes lasting a few minutes, and it worsened in the left lateral position. No h/o: diplopia, weakness, headache, dysarthria, hearing loss, tinnitus, allergies there is no history of similar illnesses in the past or in the family.
On examination: conscious, obeying commands, vitals stable. CNS: higher mental functions are normal. Cranial Nerve: Normal Tone- Normal. Muscle power: normal. Romberg signs: postural instability (+) on the left side Special test: Dix Hall pike test: torsional clockwise nystagmus (+) on the left side. Supine roll test (-). Motion sensitivity quotient: above 30 seconds (severe).
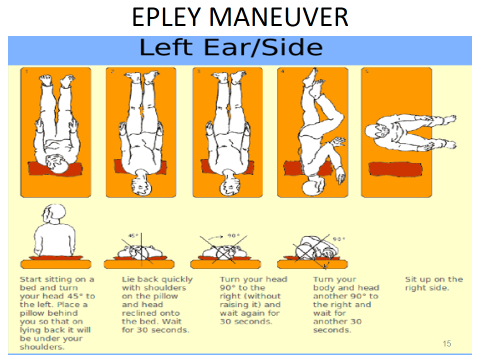
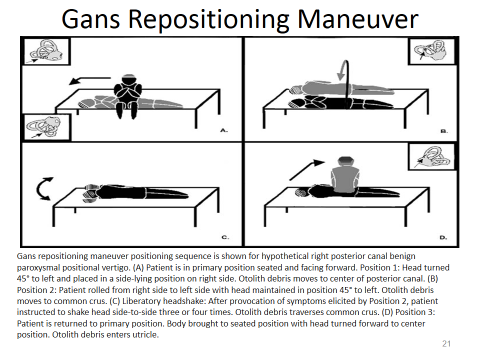
Final Diagnosis: Left posterior-Semicircular canal BPPV. Intervention of the left-sided Gans repositioning maneuver (with soft collar), balance, and gaze stability exercises were performed two times per day.
Interventions
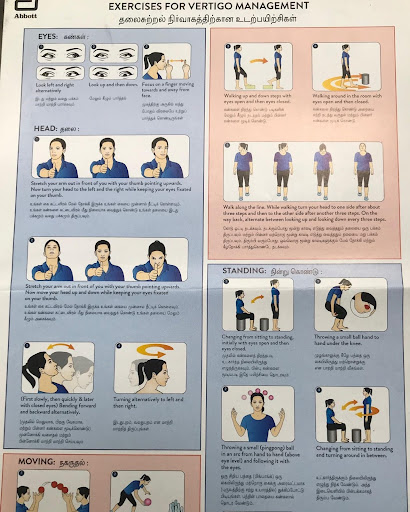
- Gaze Stability & Balance Exercises
- Epley or Canalith repositioning maneuver (Ant & Post-SCC BPPV)
- Lampert or Barbecue roll maneuver (Hz-SCC BPPV)
- Gans repositioning (Older people have Post-SCC BPPV)
Discussion
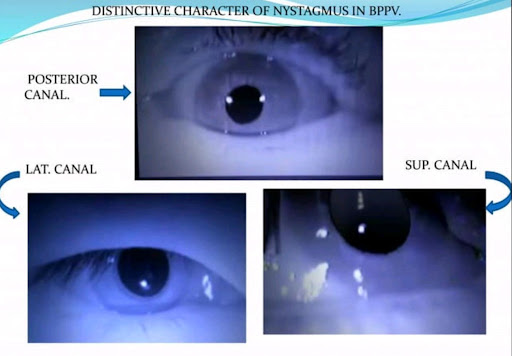
Patients were carefully screened using a detailed motion sensitivity quotient (MSQ). Then postural tests by Romberg and single-leg stance tests were done, and the postural instability was watched carefully. Then positional tests like the Dix-Hall pike and supine roll test were done, the nystagmus was watched carefully, and semicircle canal involvement was diagnosed. The posterior canal is the most commonly affected site, but the superior and horizontal canals can be affected as well. It should be noted that the superior canal is sometimes also referred to as the anterior canal, and the horizontal canal is sometimes referred to as the lateral canal.
The Dix-Hall pick test was used to diagnose posterior and anterior canal BPPV, and therapeutic Epley maneuver is used. For horizontal canal BPPV, the diagnosis maneuver is a supine roll test, and the therapeutic barbecue roll maneuver is used. Gaze stability exercises for nystagmus and balance exercises can help you improve stability and prevent fall risks. For elderly patients with posterior semicircular canal BPPV facing challenges from coexisting cervical spondylosis, a safety measure to prevent neck pain is recommended.
Physical therapy outcomes should also include teaching the patient how to use the appropriate techniques at home to prevent recurrences. Challenges faced by patients, such as reduced activity levels and quality of life. It has been estimated that 30% of elderly patients experience a balance disorder. Challenges encountered while doing therapeutic maneuver trigger dizziness that will be eliminated by avoiding movements such as looking up or sitting immediately and skipping seconds of head changing position while doing maneuver. These are the factors that bring on the symptom of feeling dizzy. Managing these disorders is a substantial challenge for patients, their careers, and physicians.
Challenges behind while performing therapeutic maneuver, for each position change, it takes about 30 to 60 seconds for the crystals to settle into the most dependent position in the canal. If turns are made before the crystal has a chance to settle, the crystal may fall back the wrong way, and the maneuver will fail to work. It is also important that each of the head positions be fully turned, or else the crystals will not settle to the correct position in the canal and the maneuver will fail. Also, if the position changes are done too slowly, the crystals may not settle quickly enough from a lack of momentum, and the maneuver will fail once the crystal falls out of the canal. Essential seconds of head holding and momentum are achieved when the head is moved in such a way to manipulate the crystal to fall towards the canal opening and settle back to the utricle and the maneuver leads to success.
Conclusion
Patients were followed up on the 14th day, and one month later.
The clinical outcome for adult and middle-aged patients: Symptoms reduced within 1-2 weeks; and for older patients, the symptoms reduced after four weeks, and finally achieving good quality of life.
A correct diagnosis is important to identify the affected side of the semicircular canal involvement and to adopt the most appropriate therapeutic maneuvers to obtain a good therapeutic outcome in this atypical form of BPPV.
Home Advices
- Before performing therapeutic maneuver, horizontal movement of the head should be performed to prevent stiff neck muscles.
- Sit down at once if you feel dizzy.
- Use good lighting if you get up at night.
- Use a Cervical Collar while exercising only for older people.
- Avoid sleeping on the affected side.
- Avoid sudden jerky head movements.
- Sleep with your head elevated about 45 degrees, in daytime sit in the EC chair for one week.
- When you wake up in the morning, lift your head slowly and sit on the side of the bed for a moment before you stand up.
- After doing the maneuver, don’t change the position; sit for five minutes.
Reference
1. O’Sullivan, et al. Physical Rehabilitation. 6th Edition, FA Davis Company, Philadelphia, 2014, 108-109.

GK. Balasubramani,
Senior Physiotherapist