Bentalls Procedure
Kanimozhi1,*, Pushpa2,
1OT Assistant Manager, Kauvery Heartcity, Trichy, India
2OT Incharge, Kauvery Heartcity, Trichy, India
*Correspondence: nursing.heartcity@kauveryhospital.com
Abstract
A 22 years old male came with complaints of breathing difficulty. He received the Bentall procedure + residual VSD closure.
Background
A Bentall procedure is a surgery to help correct problems with the root of aorta, usually an aneurysmal dilatation; the Aortic valve may also be abnormal, and usually has regurgitation. Aortas role is to carry oxygen rich blood from the heart to the rest of our body. It is sized at around 30 centimeter long and 2.5cm width. The aorta is the largest artery in our body.
Risk factors
| Predisposing condition | Pain characteristics | Physical exam findings |
| Marfan Syndrome | Abrupt onset of pain | Hypertension |
| Family History of aortic disease | Severe pain intensity | May have pain + breathing difficulty |
| Known aortic valve disease | Ripping or tearing pain | New aortic insufficiency murmur + pain |
| Known thoracic aortic disease | – | Pulse deficit
BP differential 20mm/Hg |
| Bicuspid aortic valve | – | |
| Smoking and cocaine use | – |
Aortic Disease and managment
| Type A | Type B | |
| Description | Dissection of ascending or proximal aorta | Dissection of descending or distal aorta |
| Treatment | Open repair of aorta to remove entry into false lumen | Medial management for uncomplicated dissection endovascular or open repair |
| Aim of Treatment | Prevent aortic rupture prevent development of pericardial effusion and cardiac tamponade | Prevent aortic rupture |
| Indication for surgical treatment | Always indicated | Persistent or recurrent chest pain, mal perfusion, expansion of aortic diameter |
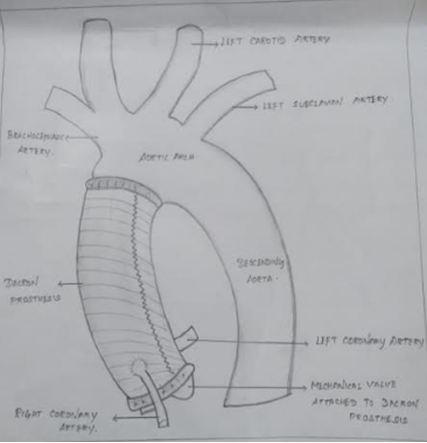
Bentall Diagram:
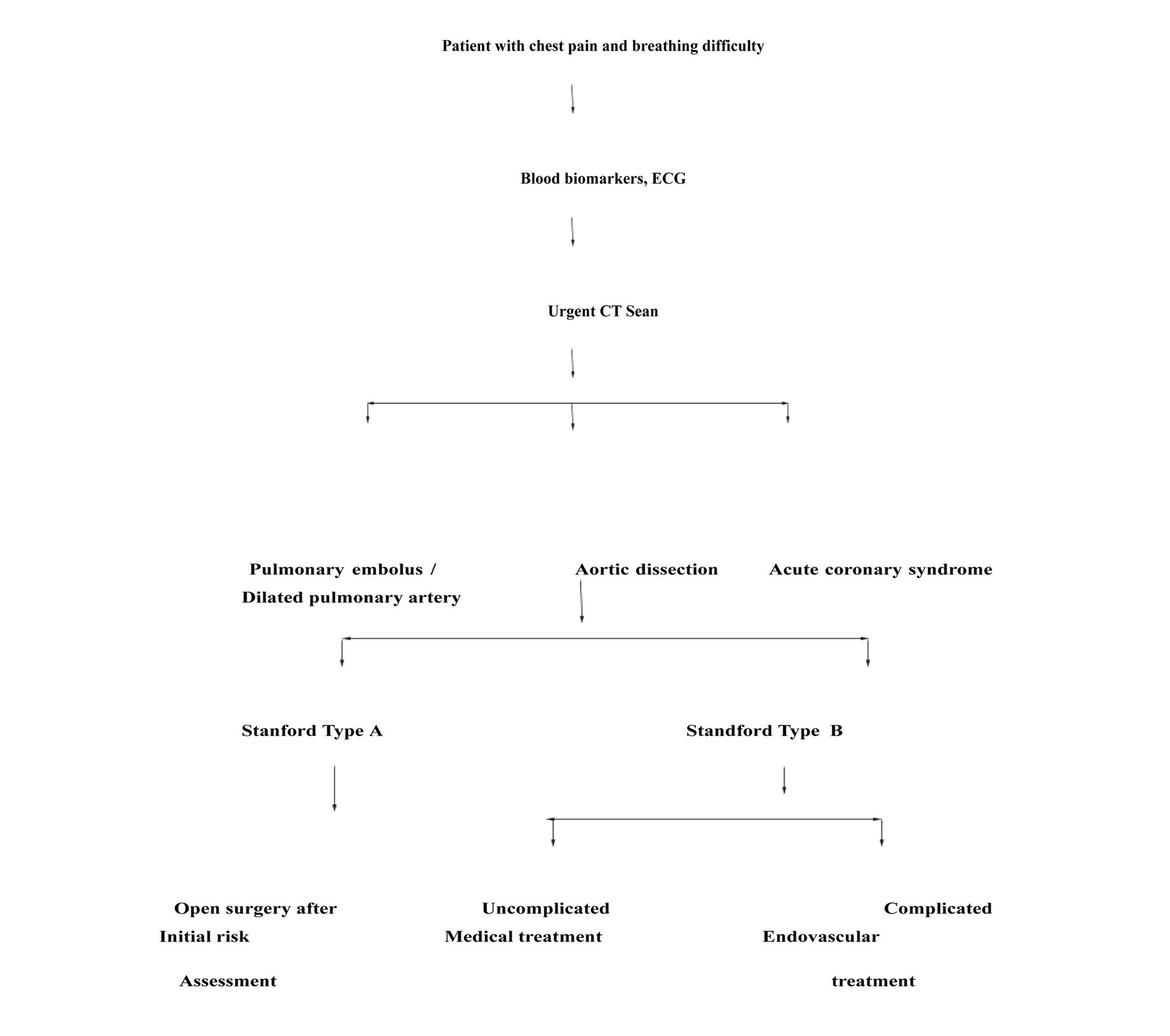
Clinical pathway to Bentall
Case Presentation
On admission patient had complaints of breathing difficulty and then came for Bentall procedure + residual VSD closure.
On Examination
ECHO
- S/P VSD surgical closure
- 3mm residual peri-membrane
- Type of VAD with left to right shunt
- Severe AR
- Concentric LVH
- Normal LV systolic function
- EF: 69%
CT scan of Aortic Angio report
- K/C/O Closure status
- Cardio megaly, with dilated pulmonary artery
- Gross dilation of the aortic root and ascending aorta
- No evidence of dissection
- Bilateral basal atelectasis
Pre op Medication:
Nil Drugs
Past Surgical History:
VSD closure done on 2010 (Kauvery Hospital Tennur)
Pre op Investigation:
HB : 16.1
PCI : 46.8
Urea : 27.4
Creat : 0.87
Na+ : 137
K+ : 4.5
Platelet Count : 272000
Chloride : 101.5
Bicarbonate : 26.3
Intra Operative Procedure: (Bentall + VSD gorter patch closure)
- Redo mid line sternotomy done and heparinized.
- Went on CPB with aortic an RA cannulation.
- Aorta cross clamp and heart arrested with ostial delnidu plegia.
- Patch closure of large sub aortic VSD done.
- Bentall procedure done with 21mm SJM mechanical valve in 24mm Intergard graft (composite) using interrupted suture technique.
- Distal anastomosis of graft to proximal ascending aorta done.
- Root cross clamp released.
- Came in sinus rhythm
- Weaning and de cannulation
- Chest drain and RV pacing wire placed.
Post-Operative:
0 POD (ICD 490ml)
- Patient Vital stable
- Patient received from HC OT
- ABG analysis was done
- X ray was taken
- ECG was taken
- 4th Hr ET and Oral suction was done
- 4th Hr ABG analysis was done
- 4th Hr back care was done
- Catheter care was given
1 POD (ICD 570ml)
- At morning 06:00am patient put on CPAP mode
- After consultant visit extubated was done
- After extubated 2 h ABG analysis was done
- Back care was given after extubated
- After 2 h restart oral fluid
- At 12:00am clock ABG analysis was done
- Physio and spiro was given
- Catheter care was given
II POD (ICD 340ml)
- Patient vital stable
- Chest dressing was changed
- Patient have temperature (101.2℉)
Adviced to change the antibiotic and Inj.Magnex fort 1.5gm BD added. Also adviced to take 3 set of blood culture.
III POD
- Patient vital stable
- All line removed ART, ICD
- Inj.Heparin was stopped
- CVC line was removed
- Pacing wire was cut.
- Patient transfer to ward
Post op Investigation:
| S N | Investigations | 0 POD | I POD | II POD | III POD |
| 02/06/23 | 03/06/23 | 04/06/23 | 05/06/23 | ||
| 1 | HB | 9.9 | 9.3 | 10.8 | 9.6 |
| 2 | PCV | 25 | 24 | 30.5 | 24.5 |
| 3 | Urea | 28.6 | 30.9 | 35.1 | 32.1 |
| 4 | Crea | 0.7 | 0.8 | 0.85 | 0.84 |
| 5 | Na+ | 138 | 135 | 135 | 136 |
| 6 | K+ | 3.9 | 4.0 | 3.5 | 3.9 |
| 7 | Test | – | 12.7 | 15.7 | 22.8 |
| 8 | Con | – | 11.4 | 11.4 | 11.4 |
| 9 | INR | – | 1.1 | 1.1 | 2.0 |
| 10 | TC | – | – | – | 16200 |
| 11 | CRP | – | – | 240 | – |
| 12 | Procal | – | – | 2.23 | – |
| 13 | Acitrom | – | 4 mg | 4 mg | 3 mg |
Nursing Care
- Connect patient to ventilator.
- Monitor ECG, oxygen saturation, blood pressure and blood gases.
- Check urinary output and chest tube output.
- Prior to discharge wean off ventilator train patient to incentive spirometer.
- Anticoagulation therapy, diet as tolerated and ambulation.
Nursing Diagnosis
- Decreased cardiac output related to charges in intra vascular volume hemorrhage.
- Anxiety related to fear of death sudden onset of illness as evidenced by increased alertness and restlessness.
- Deficient knowledge (pre operatively and post operatively) related to newly identified need for aortic surgery.
Nursing Management
- Managing decrease in cardiac output.
- Assess for signs of myocardial ischemia, chest pain, tachycardia or ST segment and T-valve changes on ECG.
- Assess the client hemodynamic status monitor signs of decreasing cardiac output, decreased urine output and restlessness.
- Administer medication intravenous fluid and blood as ordered.
- IF decreased cardiac output is drug induced.
- Provide non pharmacological measure to manage stress such as relaxation technique, medication and deep breathing exercises.
- Assess neurological status.
- Administer medication and pharmacologic support
- Beta blocker (metoprolol propanol)
- Calcium channel blocker (amlodipine, diltiazem)
- Angiotensin converting enzyme (losartan, Valsartan)
- Antiplatelet agent (Aspirin clopidogrel)
- Anti-hypertensive medication Hydralazine)
- Monitoring laboratory and diagnostics
- CBC
- Coagulation profile
- Lipid Profile
- Renal function Test
Diet
- Try to avoid sugary foods
- Limit your intake of salty foods, it will help prevent water retention and keep blood pressure normal.
- Water consumption it helps maintain proper fluid balance in the body.
- Limit your consumption of processed fats instead switch to healthy fats derived foam nuts, avocados seeds and fish.
- Different variety of fish such as salmon, sardines and mackerel are rich sources of omega 3 fats.
- Low fat dairy and include it in your everyday
- Include protein rich foods such as egg, nets, green leaf.
- To take whole grain food such as brown rice oats quinoa, couscous, barely, whole grain breads.
- Vitamin K rich food completely avoid after surgery.
Exercise
- Exercise increase your fitness level helps to control blood pressure, weight and cholesterol and keep you relaxed.
- Start with short and simple walks and gradually increase length and intensity.
- You can walk as much as you like as long as you feel comfortable and daily walking as few minutes.
Home Advice
- Avoid lifting weight for 3 months.
- To continue physio and Spirometry.
- To continue exercises.
- Proper review.
- To follow diet plan.
- To maintain body neat and clean in every day because to prevent SSI.

Ms. Kanimozhi
OT Assistant Manager

Ms. Pushpa
OT Incharge