Anaesthesia and morbid obesity: A systematic review
Hemalatha Iyanar
Senior Consultant, Department of Anaesthesiology, Kauvery Hospital, Chennai
Abstract
Over the past few decades, there has been an increase in the prevalence of obesity and its related complications and so, they more often require surgical interventions. The Anaesthesiologist has to be very aware of the related anatomical considerations, pathophysiological changes and the pharmacokinetic alterations. These obese patients are at increased risk of perioperative complications. Most importantly, difficult access to airway and post extubation respiratory distress. Managing such patients effectively both preoperatively and postoperatively is quite challenging. This article is an update on perioperative management of a morbidly obese patient and on the recent advances in safe and effective care of morbidly obese patients planned for surgery. For any obese patient, the implementation of protocols for mask ventilation and difficult intubation, use of protective ventilation, opioid sparing strategies and semi seated positioning throughout the care are recommended.
Keywords: Obesity, BMI, OSA, Obesity hypoventilation syndrome, difficult airway, perioperative management, Safe Apnoea Period, pharmacokinetics, ramped position, Cor Pulmonale, Deep Vein Thrombosis, Thrive, CPAP, PEEP, Apnoeic Oxygenation, Sugammadex, Rhabdomyolysis
Background
Overweight has been defined as an excess of total or expected “normal” body weight, including all tissue components (muscle, bone, water and fat) of body composition. Body mass index (BMI) is the standard measure for categorising the obesity. BMI is calculated by dividing patient weight (kg) by the square of their height (m); BMI =kg/m2.
Table 1. Classification of obesity by body mass index (BMI)
BMI | |
<20 kg/m2 | Underweight |
20-25 kg/m2 | Normal |
26-29 kg/m2 | Overweight |
30-39 kg/m2 | Obese |
≥40 kg/m2 | Morbid obese |
≥50 kg/m2 | Super-obese |
≥60 kg/m2 | Super-super obese |
World Health Organization (WHO) classification: BMI |
|
30-34.9 kg/m2 | Class I |
35-39.9 kg/m2 | Class II |
>40 kg/m2 | Class III |
Preoperative assessment
Preoperative assessments make perioperative period more efficient. A brief note on obesity and its related medical conditions would help the Anaesthesiologist to manage such patients effectively by taking more preventive measures to avoid complications and rendering them less traumatic.
Table 2. Obesity and its related medical conditions
| Organ system | |
| Respiratory | Restrictive lung disease, asthma, obstructive sleep apnoea (OSA), obesity hypoventilation syndrome (OHS) |
| Cardiovascular | Hypertension, cardiomyopathy, congestive heart failure, coronary artery disease, peripheral vascular disease, thromboembolism, sudden death |
| Endocrine/metabolic | Type 2 diabetes mellitus, Cushing’s syndrome, hypothyroidism, hyperlipidaemia, vitamin deficiencies |
| Gastrointestinal | Hiatal hernia, inguinal and umbilical hernia, fatty liver, gallbladder stones |
| Musculoskeletal | Osteoarthritis on weight-bearing joints, low-back pain |
| Malignancy | Breast, prostate, cervix, uterus, colorectal |
| Psychiatric | Depression, low self-esteem |
Preoperative evaluation should be carried out well ahead, to allow modification of perioperative management and optimization of such patients for the proposed surgery. Medical history-taking and physical examination has to be performed, focusing more on associated medical illness, airway assessment, presence of obstructive sleep apnoea (OSA), metabolic syndrome, cardiorespiratory fitness. Investigations should be tailored to the individual patient, co-existing diseases, the type and urgency of the surgery.
Table 3. Routine preop tests for obese patients
| Fasting plasma glucose |
| Lipid profile |
| Electrolytes including sodium, potassium, calcium, and phosphorus |
| Liver function tests including AST, ALT, total, and direct bilirubin |
| Renal function tests including creatinine level |
| Complete blood cell count |
| Ferritin |
| Vitamin B12 |
| Thyroid stimulating hormone (TSH) |
| 25-Hydroxy vitamin D level |
| Testosterone level |
| Electrocardiogram (ECG) |
| Especially in >55-year-old women and >45-year-old men who has established or suspected heart disease or at higher risk for heart disease |
| P-A chest X-ray |
| Especially in >60-year-old patients with established or suspected lung or heart disease |
| Polysomnography |
| Other clinically indicated additional tests, such as echocardiography |
A preoperative ECG is essential to exclude factors such as rhythm disturbances, cor pulmonale, and as a guide to the need for more extensive cardiac investigations. Patients with evidence of right ventricular hypertrophy or cor pulmonale will benefit from a period of elective noctural non-invasive ventilation before elective surgeries.
Table 4. Common ECG abnormalities associated with morbid obesity
| Low voltage complexes |
| LV hypertrophy or strain |
| Prolonged QT/QTc |
| Inferolateral T wave abnormalities |
| Right axis deviation or RBBB |
| P pulmonale |
| Conditions | Suggestive features | Actions required before surgery |
| Respiratory | ||
| Sleep-disordered breathing (OSA, OHS) | Shortness of breath | ABG initially Spirometry CPET if abnormalities found in above tests Airway planning 4x increased risk of difficult intubation and difficult mask ventilation Commence CPAP before surgery and continue after surgery BiPAP sometimes necessary for improvement in symptoms (especially OHS) Plan for postoperative HDU/ICU admission if symptoms not improved by time of surgery |
| Spo2<95% breathing air | ||
| STOP-BANG >=5 | ||
| OHS-BMI>30, hypercapnia when awake, raised HCO3, hypoxia, exclusion other causes of hypoventilation | ||
| Asthma | Dyspnoea | Asthmatic symptoms common but reversibility with β2-agonists not always found-cause is partly chronic pro-inflammatory state from excess adipose tissue, and fat within/around chest/abdomen causing small airway collapse Weight loss: symptoms from both 'classical' asthma and fat-related wheeze will improve |
| Wheezing | ||
| Cardiovascular | ||
| Hypertension | Clinical signs of heart failure | Preoperative ECG ECHO if structural or functional disease suspected Referral to cardiologist Medical management and optimisation before surgery |
| Left ventricular hypertrophy | History of cardiac syncope. Increased SBP | |
| Left ventricular failure | Reduced exercise capacity | |
| Conduction abnormalities | ||
| Cardiomyopathy | ||
| Right heart failure | Pulmonary hypertension resulting from sleep-disordered breathing | |
| Polycythaemia | ||
| Reduced functional capacity | ||
| Difficult to assess in obese patients | Assess ability to walk on a flat level surface Assess climbing stairs CPET: not routine, but can be used where assessment suggests high risk patient equipment may not tolerate patients' weights obesity can confuse interpretation of results | |
| Ability to achieve 4 METS indicates fitness and low risk patient | ||
| Metabolic | ||
| Diabetes mellitus | Deranged serum glucose, HbA1C, or associated complications | Optimise glucose control with referral to endocrinologist Avoid delaying surgery based on HbA1C concentrations only |
| Liver involvement (NASH/NAFLD) | Evidence of cirrhosis, deranged LFTs | Liver-shrinking diet (<1000 calories per day) can reverse the disease processes somewhat |
| Metabolic syndrome | Central obesity, hypertension, impaired glucose handling or DM, increased triglycerides, decreased HDL cholesterol | Actively seek components of metabolic syndrome (three or more required for diagnosis) |
Organization and equipment
Preoperative assessment should assess the ability of a patient to mobilize on the day of surgery to enable planning of equipment, personnel and identification of any potential hazards or unsuitability.
Preparation and Dignity
Obese patients are mindful of societal views about their size. Dignity is important to these patients. Ensure proper size theatre gowns, appropriately sized underwear, rooms accessible with toilets and showers. Deep vein thrombosis (DVT) risk should be assessed and prophylactic measures have to be taken.
Preanaesthetic medications
Pre anaesthetic drugs are considered to alleviate infections, gastrointestinal disturbances, post operative pain, hypercoagulation and anxiety.
Moving and positioning
Appropriate equipment suitable to transfer the patient is required. Chairs, trolleys, beds and most importantly operating tables must be safe for use upto or above the patient’s weight and must be equally safe through the full anticipated range of positions and movements required. Gel pads should be used to protect pressure points. Attention to the pressure points during anaesthesia is vital. At the end of surgery, transfer from operating table to ward bed can be facilitated with slide sheets or hover mattresses.
Monitoring
Routine monitors are used. Invasive arterial monitoring is not routine for obese patients. Non-invasive BP cuffs should be of correct size. Anaesthetic ventilators should be capable of delivering high driving pressure and able to deliver PEEP. Ultrasound visualization may be useful to facilitate successful regional blocks and in securing venous access and arterial line, if it’s difficult.
Induction
Positioning
Ramp position and recently, modified ramp position, are used to position theses obese patients to provide better intubating conditions. In the ramp position, the patient’s head and shoulders are elevated to achieve alignment of the sternal notch and external auditory meatus while in modified ramp position, the patient’s shoulders were elevated using special pillow and head was extended to the most possible range. Modified ramp position provides improved laryngeal view and eliminates the need of repositioning.
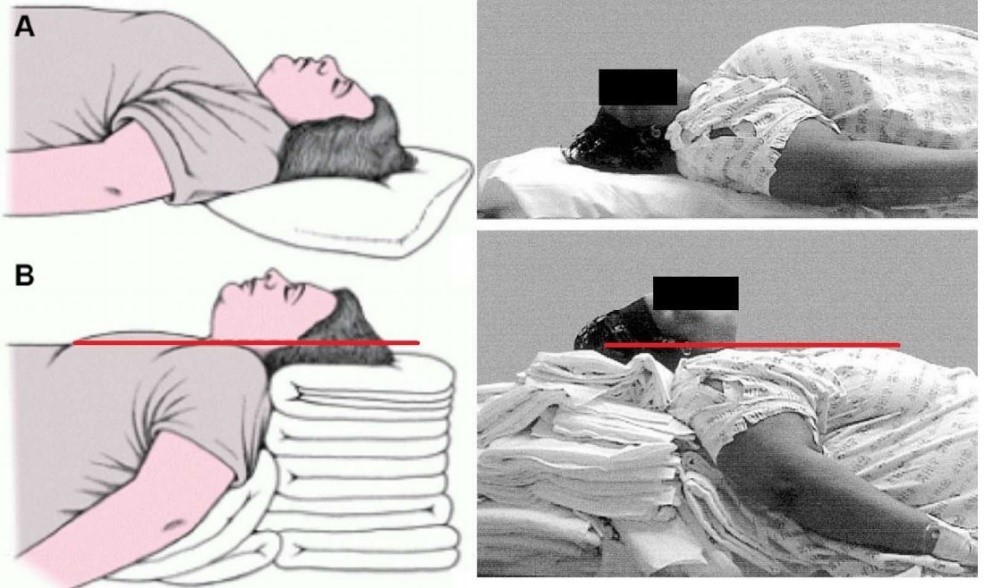
Fig. 1. RAMP position illustration – External auditory meatus in line with sternal notch.
Preoxygenation
Airway management remains a challenge for all obese patients because their extremely short safe apnoea period (SAP), that is the time between muscle paralysis and apnoea until oxyhemoglobin saturation (Spo2) drops to a potentially dangerous level. Preoxygenation with 100% oxygen via face mask is widely practiced for all patients to extend the safe apnoea period. Recently THRIVE technique is advised to extend this SAP.
THRIVE – transnasal humidified rapid insufflation ventilatory exchange- combines the benefits of apnoeic oxygenation with continuous positive airway pressure (CPAP) and gas exchange through flow dependant dead space flushing. During apnoea time, upper airway patency was maintained using jaw thrust. Another method to extend the SAP is Buccal oxygenation. Buccal o2 was administered via a modified Ring- Adair-Elwyn (RAE) tracheal tube placed inside the patient’s cheek.
Pharmacokinetics
Obesity alters pharmacokinetic parameters depending on lipid solubility and tissue distribution of the administered drug. Drug dosage should be adjusted by considering volume of distribution for loading dose and by considering clearance for maintenance dose. Using volatile agents with rapid offset of action, with low blood: gas partial co-efficient such as desflurane may limit absorption into adipose tissue, decreasing the risk of re-sedation, and thereby airway obstruction at emergence. Emergency drugs such as epinephrine and nor epinephrine are dosed according to ideal body weight. Suxamethonium according to total body weight. TIVA with propofol is preferred over volatiles due to rapid offset, reduced incidence of laryngospasm, clear headed emergence and reduced postoperative nausea and vomiting.
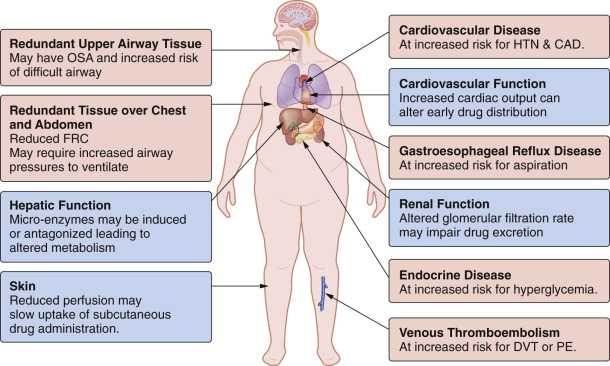
Table 6. Factors affecting drug pharmacokinetics in obesity [4]
| Volume of distribution |
| Decreased fraction of total body water |
| Increased adipose tissue |
| Increased lean body mass |
| Altered tissue protein binding |
| Increased blood volume and cardiac output |
| Increased concentration free fatty acids, cholesterol, α1 acid glycoprotein |
| Organomegaly |
| Plasma protein binding |
| Adsorption of lipophilic drugs to lipoproteins so increased free drug available |
| Plasma albumin unchanged |
| Increased α1-acid glycoprotein |
| Drug clearance |
| Increased renal blood flow |
| Increased GFR |
| Increased tubular secretion |
| Decreased hepatic blood flow in congestive cardiac failure |
Intraoperative fluid management
Obese patients undergoing surgery presents increased risk for experiencing postoperative renal failure. One proposed method is goal directed therapy (GDT) which is fluid responsiveness. Fluid responsiveness can be assessed through analysing arterial waveform. Plethysmographic waveform variation given by the pulse oximetry is also another method to analyse fluid responsiveness.
Ventilation
Recent recommendations include lung protective volumes(6-8ml/kg), plateau pressure of < 30 cm H2O, and titration of PEEP according to patient’s cardiopulmonary reserve. Patient’s intraoperative position has a significant effect on airway pressure. For upper abdominal laparoscopic procedures, patient has to be positioned in 20-degree reverse Trendelenburg with 45 degrees hip flexion. For lower abdominal lparoscopic procedures, flat Trendelenberg position is advised.
Reversal of Neuromuscular Block
Ensure complete reversal of neuromuscular block before emergence by using appropriate dose of either neostigmine or sugammadex (if rocuronium or vecuronium is used). Sugammadex is derived from cyclodextrin, and it has varying degree of affinity for different neuromuscular blocking drugs. It provides quick and complete recovery from neuromuscular blockade. Recommended dose for total reversal of intermediate or deep block is calculated based on TBW or IBW plus 40%. Sugammedex antagonism is preferred over neostigmine because of difficulties in dosing neostigmine.
Regional Anaesthesia
When appropriate, a regional anaesthesia offers advantages and should be considered in anaesthetic management plan in obese patients. Though there is an increased incidence of failed blocks in obese patients, it can be considered as a part of multimodal approach in managing postoperative pain management.
Post Operative Care
Emergence should be in 30-45 degree head up position. CPAP started in early postoperative period may enhance recovery of normal respiratory function. Utmost care should be taken to prevent the occurrence of airway obstruction and lung collapse which is very common in obese patients. Rhabdomyolysis can occur in obese patients in postoperative period. Therefore close monitoring is important for deep tissue pain and if rhabdomyolysis occur, steps should be taken to treat this condition and to prevent the occurrence of acute kidney injury (AKI).
Discharge from recovery requires
- Stable vitals with minimal oxygen requirement
- No evidence of hypoventilation
- Free from apnoea without stimulation
- Able to use CPAP device if required
Conclusion
Managing obese patients is always a challenge to Anaesthetists and delivering high quality, resource efficient care requires proper planning and optimization. Day care surgery is also a feasible option. Obesity carries risk for surgical and postsurgical complications. With appropriate collaborative efforts among medical disciplines, these complications can be reduced significantly.
References
- Obesity and overweight. (cited 2021 september 27). Available from https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight.
- Ogden CL, et al. Prevalance of childhood and adult obesity in the United States, 2011-2012.
- BMC Anaesthesiology 22, Article number :98 (2022). Available from https://bmcanesthesiol.biomedcentral.com.
- Ladosky W, et al. Chest mechanics in morbidly obese non- patients. Respir Med. 2001;95:281.
- Anaesthesia for the patient with obesity, from https://www.uptodate.com. (updated on april 05, 2022). Available from https://www.wolterskluwer.com/en/know/clinical-effectiveness-terms.
- Wynn-Hebden A, et al. Anaesthesia for the obese patient. BJA Education 2020;20(11): P388-395.
- Illustration from aneskey.com. Available from https://images.app.goo.gl/uCm4HX3CRb5TfYPy5.
- Anaesthesia and morbid obesity academic article available from https://academic.oup.com/bjaed/article/8/5/151/268305.
- Regional anaesthesia and obesity by National library of medicine, October 2009, available from https://pubmed.ncbi.nih.gov.
- Obesity and Anaesthesia management, published: February 08, 2017, available from www.intechopen.com.
- Perioperative care of the obese patients available from www.bjssjournals.onlinelibrary.wiley.com.
- Recent advances in Anaesthesia of the obese patient by Jay B. Brodsky available from https://pubmed.ncbi.nlm.nih.gov.

Dr. Hemalatha Iyanar
Senior Consultant