Prevalence of vitamin B12, folate deficiency and homocysteine elevation in ASCVD or venous thrombosis
Dominic Rodrigueza,*, Stephy Georgeb,*
aConsultant Physician, Kauvery Hospital, Trichy
bResident General Medicine, Kauvery Hospital, Trichy
*Correspondence: domappa1966@gmail.com (D. Rodriguez); stephyg2386@gmail.com (S. George)
Abstract
Background: Vitamin B12 and folate are essential components for the metabolism of homocysteine. Elevated homocysteine has been associated with increased risk of atherosclerotic cardiovascular disease. The aim of the study is to evaluate the prevalence of vitamin B12, folate deficiency and hyperhomocysteinemia in patients presenting with any atherosclerotic cardiovascular disease or venous thrombosis.
Methods: Sixty-five patients who presented with any ASCVD or venous thrombosis were included in the study. Detailed history including BMI and diet history were taken. Blood samples were collected and sent for vitamin B12, folic acid and homocysteine analysis. Hematological parameters including Hb, MCV, MCH, MCHC were studied.
Results: Homocysteine was elevated in 70.77% of patients. Vitamin B12 was deficient in 47.69% of patients. Folate deficiency was much higher 61.54%. A 43% of the patients who had vitamin B12 deficiency and homocysteine elevation. A 53.85% of the patients with folate deficiency had homocysteine elevation. There was moderate negative correlation between vitamin B12 and homocysteine and a weak negative correlation between folate and homocysteine.
Keywords: Homocysteine, Vitamin B12, Folate deficiency, Atherosclerotic cardiovascular disease, Thrombosis, CAD, Risk factor
Background
Homocysteine is a sulphur containing amino acid formed by demethylation of essential amino acid methionine. Vitamin B12 and folate are essential components in the metabolism of homocysteine [1]. Low B12 and folate levels are common in Indians particularly in vegetarians.
Hyperhomocysteinemia has been associated with increased risk of atherothrombotic vascular events [2]. Increased homocysteine levels lead to endothelial dysfunction, stimulate inflammation, oxidative stress and induction of a procoagulant environment [3–6]. The aim of the study is to evaluate the prevalence of vitamin B12, folate deficiency and hyperhomocysteinemia in patients presenting with any atherosclerotic cardiovascular events.
Methods
This is an observational study of 65 patients who are admitted with atherosclerotic cardiovascular disease (ASCVD) or venous thrombosis in Kauvery Hospital, Trichy from July 2019 to July 2020. Detailed history including body mass index (BMI) and diet history were taken. Blood samples were collected and sent for vitamin B12, folic acid and homocysteine analysis. Hematological parameters including Hb, MCV, MCH, MCHC were studied. Data was entered on Microsoft Excel and analysed.
Results
Sixty-five patients who are presented with ASCVD, homocysteine elevated in patients up to 70% (Table 1). Vitamin B12 deficiency was found 7.6% (Table 2). The prevalence of folic acid deficiency was much higher 61% (Table 3). We observed a moderate negative correlation between vitamin B12 and homocysteine elevation. Also there was a negative correlation between folate and homocysteine elevation. ACS was the most common presentation in our study followed by CVA. Though majority of the patients had arterial thrombosis, the incidence of homocysteine elevation was higher in venous thrombosis (73.9%).
Table 1. Descriptive analysis of homocysteine in the study population (N = 65).
| Homocysteine | Frequency | Percentage (%) |
|---|---|---|
| Normal | 19 | 29.23 |
| Elevated | 46 | 70.77 |
Table 2. Descriptive analysis of vitamin B12 in the study population (N = 65).
| Vitamin B12 | Frequency | Percentage (%) |
|---|---|---|
| Normal | 34 | 52.31 |
| Deficient | 31 | 47.69 |
Table 3. Descriptive analysis of folate in the study population (N = 65).
| Vitamin B12 | Frequency | Percentage (%) |
|---|---|---|
| Normal | 25 | 38.46 |
| Deficient | 40 | 61.54 |
Table 4. Descriptive analysis of vitamin B12 deficiency and homocysteine elevation in the study population (N = 65).
| Vitamin B12 deficient and homocysteine elevated | Frequency | Percentage (%) |
|---|---|---|
| Yes | 28 | 43.08 |
| No | 37 | 56.92 |
Table 5. Descriptive analysis of folate deficiency and homocysteine elevation in the study population (N = 65).
| Folate deficient and homocysteine elevated | Frequency | Percentage (%) |
|---|---|---|
| Yes | 35 | 53.85 |
| No | 30 | 46.15 |
Table 6. Correlation of homocysteine with vitamin B12 and folate (N = 65).
| Parameter | Spearman correlation (rs) | P-value |
|---|---|---|
| Vitamin B12 | – 0.523 | < 0.001 |
| Folate | – 0.385 | 0.002 |
There was moderate negative correlation between vitamin B12 and homocysteine. (rs value: – 0.523 & P-value: < 0.001). There was weak negative correlation between folate and homocysteine. (rs value: – 0.385 & P-value: 0.002) (Table 6, Figs. 1 and 2).
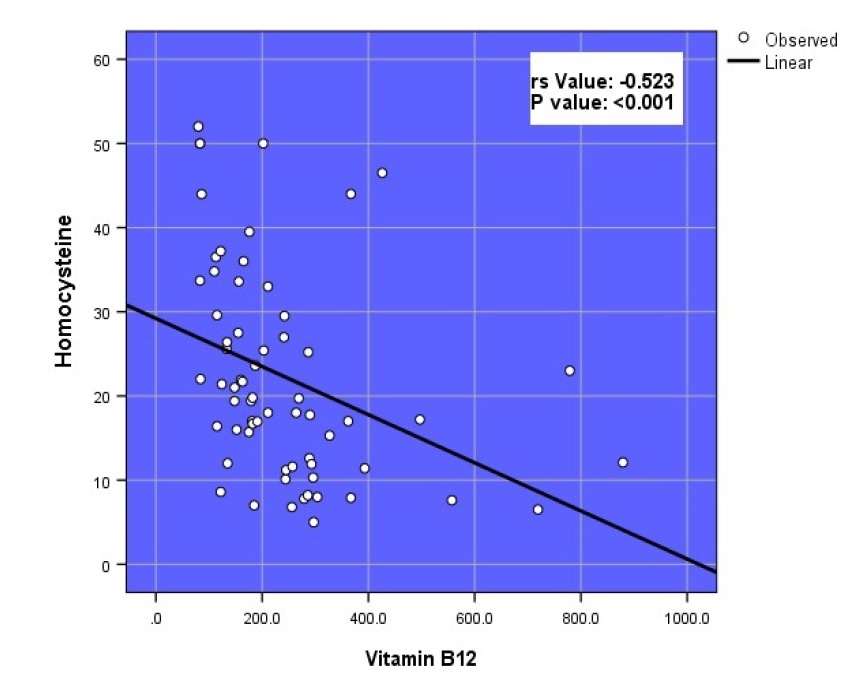 Fig. 1. Scatter plot of homocysteine and vitamin B12 (N = 65).
Fig. 1. Scatter plot of homocysteine and vitamin B12 (N = 65).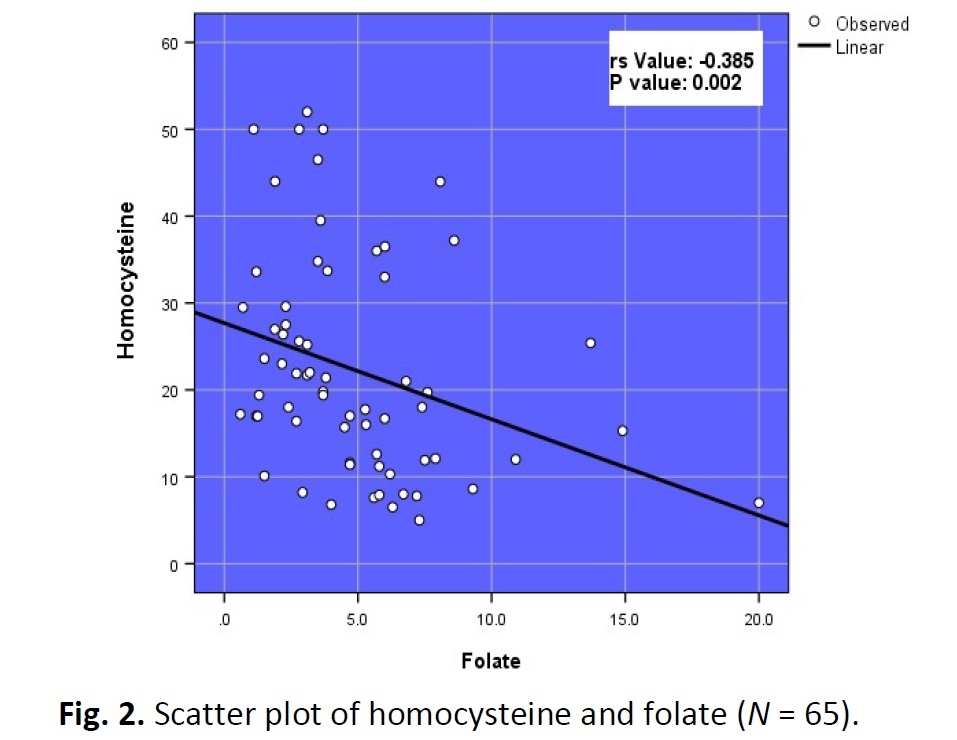 Fig. 2. Scatter plot of homocysteine and folate (N = 65).
Fig. 2. Scatter plot of homocysteine and folate (N = 65).Table 7. Linear regression analysis of factors influencing homocysteine in study population (N = 65).
| Parameter | Regression coefficient | 95% CI Lower / Upper |
P-value |
|---|---|---|---|
| Vitamin B12 | -0.027 | -0.045 / -0.009 | < 0.003 |
| Folate | -1.107 | -1.972 / -0.241 | 0.013 |
With unit increase in vitamin B12, there is a 0.027 decrease in homocysteine and is statistically significant with P-value 0.003. (95% CI -0.045 to -0.009). With unit increase in folate, there is 1.107 decrease in homocysteine and it was statistically significant with P-value of 0.013. (95% CI -1.972 to -0.241) (Table 7).
Table 8. Comparison of diagnosis between homocysteine (N = 65).
| Diagnosis | Homocysteine Normal (N = 19) |
Elevated (N = 46) |
|---|---|---|
| ACS | 10 (52.63%) | 10 (21.74%) |
| CVA | 3 (15.79%) | 9 (19.57%) |
| CVT | 4 (21.05%) | 10 (21.74%) |
| DVT | 1 (5.26%) | 7 (15.22%) |
| PTE | 0 (0%) | 4 (8.7%) |
| DVT With Pte | 0 (0%) | 2 (4.35%) |
| Other Thrombosis | 1 (5.26%) | 4 (8.7%) |
Among the participants with elevated homocysteine, 10 (21.74%) of the participants had ACS, 9 (19.57%) of the participants had CVA, 10 (21.74%) had CVT, 7 (15.22%) of the participants had DVT, 4 (8.7%) had PTE, 2 (4.35%) of the participants had DVT with PTE and 4 (8.7%) of the participants had other thrombosis (Table 8).
Discussion
Hyperhomocysteinemia is found to be positively associated with ASCVD and venous thrombosis [7– 10]. It has been postulated that higher homocysteine levels lead to epigenetic modification by macromolecular global DNA methylation, which is associated with CAD in Indian patients [11–12]. The association of hyperhomocysteinemia with CAD seems stronger in Indian patients [13]. Hyperhomocysteinemia has been reported in Indian children and adolescents and found to be related to atherogenic dyslipidemia. Hence homocysteine levels are an important determinant of cardiovascular risk factors in Indians with or without CAD [14–17].
Out of 65 patients, 51 were males (78%) and 14 were females (21%) which showed a male preponderance for ASCVD. A study of 300 patients with CAD, 216 were men (72%), 84 were women (28%) showed a higher prevalence for cardiovascular disease in males [18].
The mean age in our study population was 46.65 ± 9.67. The upper limit of age was 60-years-old.
Mean BMI in our study was 24.26 ± 2.95. The 32 patients (49.2%) were found to be overweight (BMI 25 – 30) and 2 patients were found to be obese (BMI > 30). Among 34 patients, the 29 patients (BMI > 25) had elevated homocysteine (85.2%). In a case control study by Anan et al [19] reported higher BMI and waist hip ratio in the group with high homocysteine as compared to a group with normal homocysteine levels.
Mean homocysteine in our study population was 22.28 ± 12.54. A higher level was noted in the study conducted by Mahelle et al. [18], where the mean homocysteine level was 36.5 ± 13.58.
Forty-six patients (70.7%) who presented with ASCVD had homocysteine elevation. Mahalle et al. [18] showed hyperhomocysteinemia was present in 95.3% patients with CAD.
Yagnik et al. [20] studied 441 men in rural and urban Indians, 79% had hyperhomocysteinemia which was comparable to our study. In a case control studied by Sadeghian et al. [21] which included 294 individuals with premature CAD, prevalence for hyperhomocysteinemia was 47.4%.
In our study, vitamin B12 deficiency was found in 31 patients (47.6%). The prevalence of folate deficiency was much higher (61%). The study conducted by Mahalle et al. [18], showed the prevalence of vitamin B12 was higher (86.7%) and folate was 2.7%. They concluded that vitamin B12 deficiency and hyperhomocysteinemia are related with cardiovascular disease in Indian patients with CAD. Our findings suggested that folate deficiency has important implication in vascular events.
In our study, 35 patients (53.8%) with folate deficiency had homocysteine elevation which was higher than vitamin B12. The 28 patients (43%) who had vitamin B12 deficiency had homocysteine elevation whereas the rest 37 patients (56%) who had vitamin B12 deficiency had a normal homocysteine.
In our study majority had arterial thrombosis. But the incidence of homocysteine elevation was higher in venous thrombosis. Of the 23 patients who presented with venous thrombosis, 17 patients had homocysteine elevation (73.9%). All the patients who had DVT had homocysteine elevation which was a significant finding in our study.
We have observed a moderate negative correlation between vitamin B12 and homocysteine elevation P-value < 0.001. But there was a negative correlation between folate and homocysteine elevation P-value 0.002. This was similar to the study by Mahalle et al. [18], where homocysteine was inversely associated with vitamin B12 (R = – 0.285, P-value < 0.001). But folate did not show an inverse correlation.
Out of patients presenting with ACS, 10 (21.7%) had elevated homocysteine and an equal number had a normal homocysteine level. Of the patients presenting with CVA, majority had homocysteine elevation (75%).
In venous thrombosis the proportion of patients with elevated homocysteine was higher. In DVT and PTE with DVT, all of them had elevated homocysteine.
Conclusion
We set out to study the prevalence of homocysteine elevation and B12, folate deficiency in all patients below the age group of 60 years’ old who presented with any form of acute arterial or venous occlusion in the real life setting. Homocysteine elevation was noted in 70.77% of the entire study population. B12 and folate deficiency was noted in 75.3% of the study population. A significant positive correlation was noted between homocysteine elevation and B12, folate deficiency. Our study population also showed the prevalence of folate deficiency, with folate deficiency being more than B12 deficiency which was statistically significant. Consistent association of homocysteine elevation was noted in venous thrombosis as opposed to arterial thrombosis (ACS/CVA). Testing vitamin B12, folate and homocysteine levels especially in patients who present with any form of venous thrombosis could be recommended. It appears to be an attractive proposition to correct nutritional deficiencies, (B12/folate) with other risk factor modification to prevent all forms of arterial and venous thrombosis.
Limitations
We have not taken a control group. Further studies involving a larger sample size will be required to investigate the benefits from vitamin administration in patients with increased homocysteine levels to prevent the incidence of ASCVD.
References
- Ng KC, Yong QW, Chan SP et al. Homocysteine, folate and vitamin B12 as risk factors for acute myocardial infarction in a southeast Asian population. Ann Acad Med Singapore. 2002;31:636- 640.
- Ganguly P, Alam SF. Role of homocysteine in the development of cardiovascular disease. Nutr J. 2015;14:6.
- Daniel GH, Sonia SA. Emerging risk factors for atherosclerotic vascular disease. A critical review of the evidence. JAMA. 2003;290:932-940.
- Stamler JS, Osborne JA, Jaraki O et al. Adverse vascular effects of homocysteine are modulated by endothelium-derived relaxing factor and related oxides of nitrogen. J Clin Invest. 1993;91:308-18.
- Lentz SR. Mechanisms of homocysteine-induced atherothrombosis. J Thromb Haemost. 2005;3:1646-54.
- Hofmann MA, Lalla E, Lu Y et al. Hyperhomocysteinemia enhances vascular inflammation and accelerates atherosclerosis in a murine model. J Clin Invest. 2001;107:675-83.
- Rees MM, Rodgers GM. Homocysteinemia: association of a metabolic disorder with vascular disease and thrombosis. Thrombosis Res. 1993;71:337-359.
- Boushey CJ, Beresford SA, Omenn GS, Motulsky AG. A quantitative assessment of plasma homocysteine as a risk factor for vascular disease: probable benefits of increasing folic acid intakes. JAMA. 1995;274(13):1049-57.
- Graham IM, Daly LE, Refsum HM, Robinson K, Brattström LE et al. Plasma homocysteine as a risk factor for vascular disease: The European Concerted Action Project.JAMA. 1997;277(22):1775-81.
- Ueland PM, Refsum H, Beresford SA, Vollset SE. The controversy over homocysteine and cardiovascular risk.The American journal of clinical nutrition.2000 ;72(2):324-32.
- Loscalzo J, Handy DE. Epigenetic modifications: Basic mechanisms and role in cardiovascular disease ( 2013 Grover Conference series). Pulmonary circulation. 2014;4(2):169-74.
- Harvey RA, Ferrier DR. Lippincott’s Illustrated Reviews, Biochemistry. 2011. p. 264–5.
- Refsum H, Yajnik CS, Gadkari M, Schneede J, Vollset S Eet al. Hyperhomocysteinemia and elevated methylmalonic acid indicate a high prevalence of cobalamin deficiency in Asian Indians. The American journal of clinical nutrition. 2001;74:233-41.
- Misra A, Vikram NK, Pandey RM, Dwivedi M et al. Hyperhomocysteinemia, and low intakes of folic acid and vitamin B12 in urban North India. European journal of nutrition. 2002;41:68- 77.
- Clarke R, Daly L, Robinson K, Naughten E et al. Hyperhomocysteinemia: an independent risk factor for vascular disease. New england journal of medicine. 1991;324:1149-55.
- Mayer EL, Jacobsen DW, Robinson K. Homocysteine and coronary atherosclerosis. Journal of the American College of Cardiology. 1996;27:517-27.
- Verhoef P, Stampfer MJ, Buring JF, Gaziano JM et al. Homocysteine metabolism and risk of myocardial infarction: relation with vitamins B6, B12, and folate. American journal of epidemiology.1996;143:845-59.
- Mahalle N, Kulkarni MV, Garg MK, Naik SS. Vitamin B12 deficiency and hyperhomocysteinemia as correlates of cardiovascular risk factors in Indian subjects with coronary artery disease. Journal of cardiology. 2013;61(4):289-94.
- AnanF, MasakiT, Yoshikazu Umeno et al. Correlation between homocysteine levels and atherosclerosis in Japanese type 2 diabetic patients. Metabolism. 2007; 56(10):1390-1395
- Yagnik CS, Deshpande SS, Lubree HG et al. Vitamin B12 deficiency and hyperhomocysteinemia in rural and urban Indians. J Assoc Physicians India 2006;54:775-82
- Sadeghian S, Fallahi F, Salarifar M, et al. Homocysteine,vitamin B12 and folate levels in premature coronary artery disease. BMC cardiovascular diseases. 2006;6:38