Frozen Elephant Trunk (FET) Procedure in a 52 years old Chronic Aortic Dissection patient
Anton Prem Thilak1,*, Venkatesa Kumar Anakaputhur Rajan1, Chandrasekar Purushothaman2, Arun kumar Govindarajan2, Siva Kumaran Subbarayan2, Harikrishnan Subramanian2, Raghuram Arani Raghavendrarao1, R. Anantharaman1
1 Department of Cardiothoracic Surgery, Kauvery hospital, Alwarpet, Chennai
2 Department of Cardiac Anaesthesia, Kauvery hospital, Alwarpet, Chennai
Correspondence: premthilak87@gmail.com
Abstract
Aortic dissection is a life-threatening condition and when it involves the entire Aorta, it’s a disease with extremely high morbidity and mortality if timely intervention not done. In this case report we discuss about a 52-year-old gentleman who developed extensive Aortic Dissection and had to undergo 2 open surgeries and 1 endovascular repair to repair the entire Aorta. We also discuss about the evolution of Aortic dissection surgeries and intricacies of Frozen Elephant Trunk operation. Frozen Elephant Trunk operation using Thoraflex Hybrid (TERUMO) prosthesis was done for this patient. Followed by that, TEVAR using valiant captiva Medtronic device was done to address the diseased distal Descending Thoracic Aorta and Abdominal Aorta. This complex procedure resulted in symptom free patient and also addressed the risk of aortic aneurysmal rupture.
Background
Surgeons continue to face significant challenges when dealing with thoracic aortic aneurysms, especially when the enlargement of the ascending aorta and arch extends beyond the left subclavian artery. Treating such cases typically necessitates either a two-step approach employing the “elephant trunk” technique or a single-stage procedure that is both extensive and potentially traumatic, often necessitating a clamshell incision. The life expectancy of untreated patients with Aortic aneurysm regardless of etiology and location, is limited, with death occurring within 5 years from rupture in more than 75% of patients
6
. In this case report we discuss about a patient who underwent Redo Frozen Trunk Procedure followed by TEVAR.
Case Presentation
A 52-year-old gentleman, known diabetic and hypertensive on medication, developed acute type A aortic dissection two years back. It was complicated with left MCA territory infarct and acute kidney injury. He underwent emergency ascending aorta replacement elsewhere. He recovered from the stroke with residual weakness in left forearm. He was also on medication for post stroke seizure.
After which, he was asymptomatic until last 3 months. He developed chest discomfort and giddiness since last 3 months for which he was evaluated. CT aortogram revealed chronic dissection flap in the arch of aorta extending into left subclavian artery, right brachiocephalic artery and distally extending upto the external iliac on the right and common iliac on the left. Celiac artery, superior mesentric artery and right renal artery were arising from the true lumen whereas Inferior mesentric artery and left renal artery were arising from the false lumen. There was partial thrombosis of the false lumen and true lumen’s diameter at D10 level was 7 mm. After necessary preoperative workup, he was planned for total arch replacement with frozen elephant trunk operation.
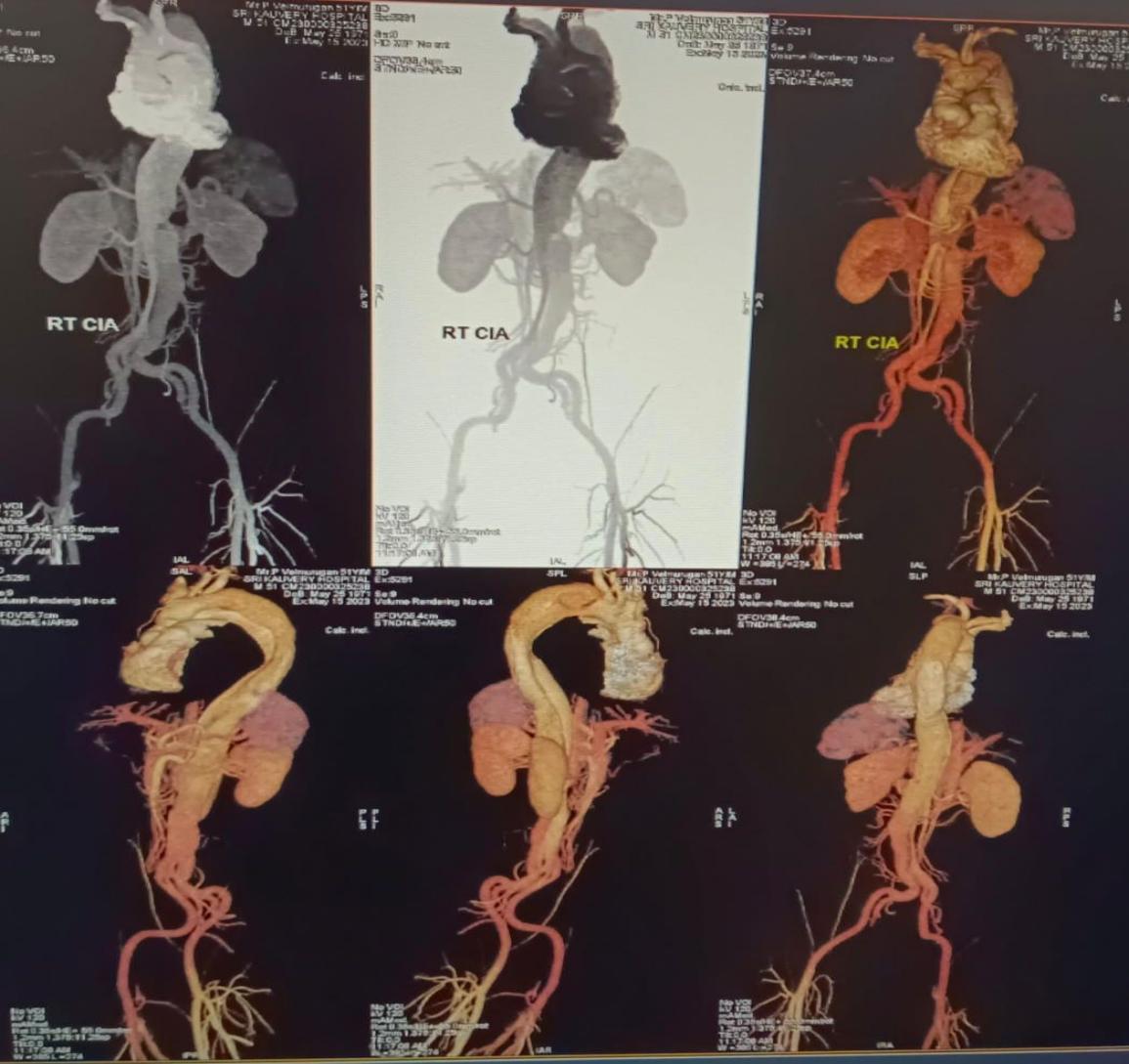
Fig. 1.
CT Aortogram showing Chronic Aortic Dissection involving the Aortic arch and extending till the bifurcation of the Iliac artery bilaterally.
Procedure
A stiff wire was passed across the true lumen of the aorta from the right femoral artery under fluoroscopy guidance. This wire was used to guide the FET graft into the true lumen. The right carotid artery (8 mm graft stitched to it) and right femoral vein were cannulated for peripheral CPB. Due to close proximity of the innominate vein and right ventricle to the posterior table of the sternum, sternotomy was performed after initiating peripheral bypass. Dense adhesions were released.
The SVC and IVC were cannulated due to insufficient drainage from the femoral vein. The aortic arch was dissected and all the arch vessels were looped. The patient’s core temperature was cooled to 25 degrees C initially and later to 19 degrees C. The cross clamp was applied and the heart was arrested in diastole by delivering custodial cardioplegia through the aortic root. Total circulatory arrest was initiated and the distal ascending aorta was transected. All the arch vessels were ligated and divided.
Antegrade cerebral perfusion was initiated through the right carotid artery, left common carotid artery, and left subclavian artery. The FET graft (Thoraflex – TERUMO) was introduced across the guide wire that was retrieved from the descending thoracic aorta. The FET graft was positioned and deployed in the descending thoracic aorta.
The sewing collar of the graft was stitched to the proximal descending thoracic aorta after reinforcing the proximal descending thoracic aorta with felt using 4-0 prolene continuous suturing. The proximal portion of the graft was anastomosed to the old ascending aorta graft using 3-0 prolene. All the arch vessels were anastomosed to the separate arms of the graft using 5-0 prolene continuous suturing.
Total body perfusion was initiated and rewarming was done. The heart regained contractions in sinus rhythm. CPB was gradually weaned off and the patient was decannulated. The chest was closed primarily on the same day.
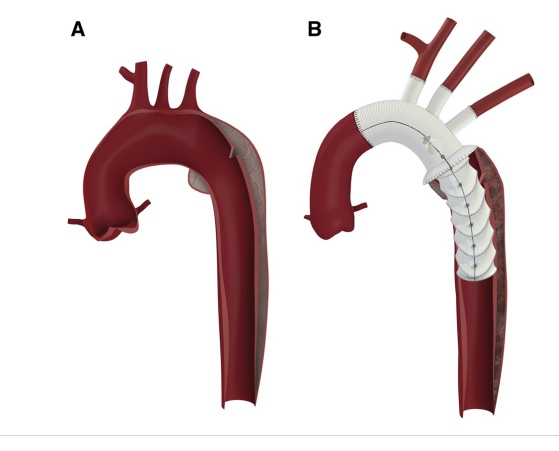
Fig. 2.
Concept diagram of Frozen Elephant Trunk (FET) procedure using Thoraflex (TERUMO) Hybrid graft.
Postoperative period
He was extubated after 15 hours of ventilation. He drained about 430 ml in the first 24 hours. He had two episodes of generalized seizure for which neurology opinion was obtained and his antiepileptic drugs were increased. He developed paralytic ileus in the second postoperative day and recovered in the fourth POD. He was shifted to the ward on 4th postoperative day, drains were removed on the next day. The patient developed intermittent fever on pod 8, two sets of blood and urine culture were aseptic. Considering the massive blood transfusion that he had during surgery, he was treated with single course of antimalarial therapy following which, he recovered from the fever. His further postoperative period was uneventful. Repeat CT aortogram showed patent conduits, no graft leaks, near complete thrombosis of false lumen of descending thoracic aorta and minimal periaortic fluid collection.

Fig. 3.
CT Aortogram of the patient after FET procedure showing well positioned stented graft in the proximal DTA and the presence of the true lumen and false lumen distal to the stented graft.
Since the true lumen diameter at level of distal Descending Thoracic Aorta was only 6mm and there was subacute thrombosis causing renal infarct in left kidney arising from false lumen, TEVAR was planned immediately. He underwent TEVAR with 32 x 28 x 150 mm valiant captiva Medtronic device. The stent was deployed just above the celiac origin (distal end) and overlaying 5 cm of FET DTA graft (above). Post deployment angiogram showed patent arteries to visceral organs. Postprocedure period was uneventful. He was discharged on 30th postoperative day.
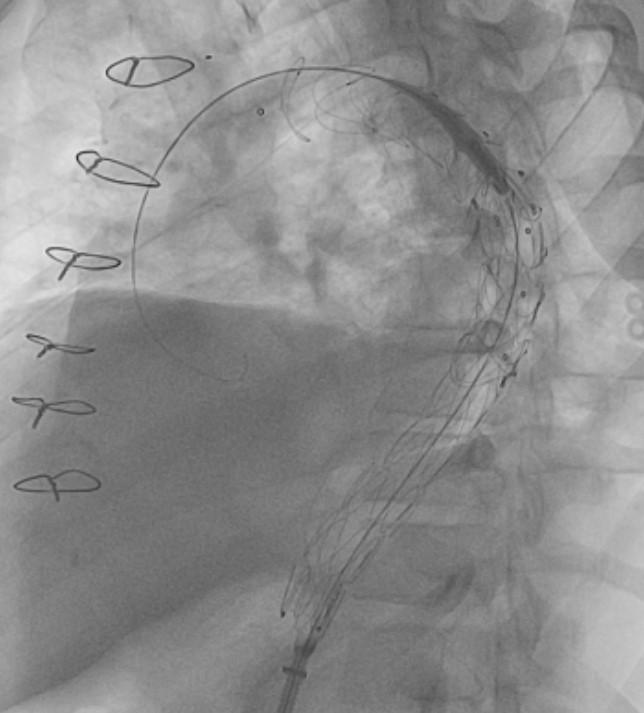
Fig. 4.
Fluoroscopy image of the patient post TEVAR deployment. Note the overlapping of the Endovascular graft over the Frozen Elephant Trunk surgically deployed.
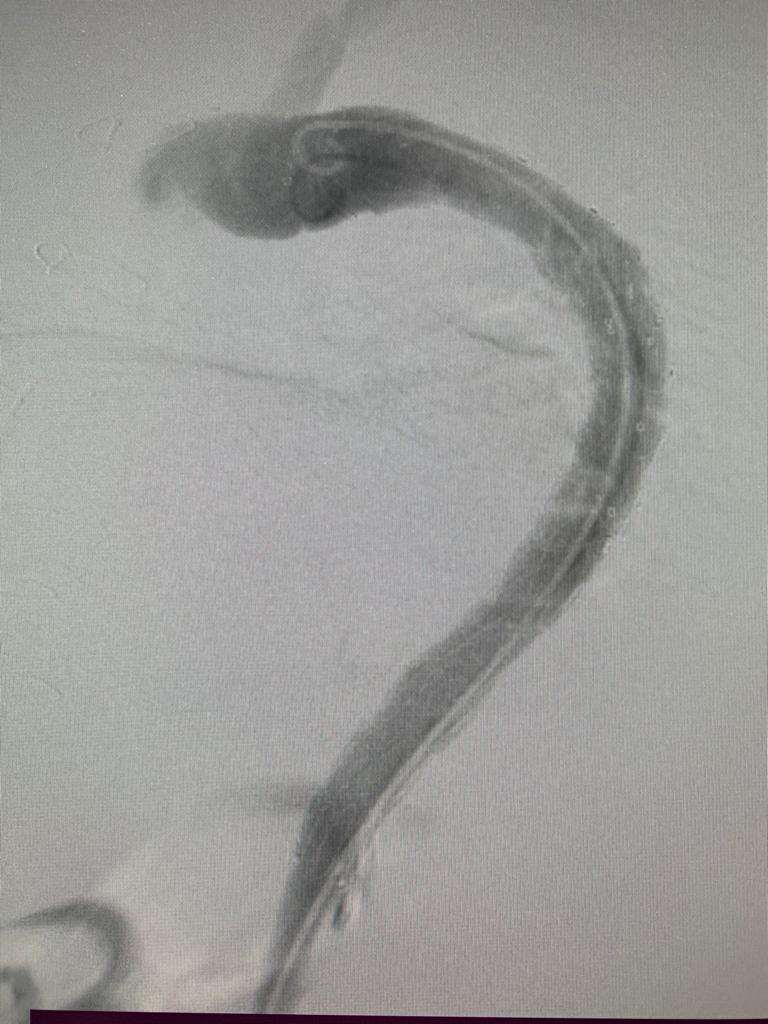
Fig. 5.
Angiography showing completely repaired DTA following FET and TEVAR.
Discussion
Aortic Dissection and aneurysm involving the Aortic arch and descending thoracic aorta have always remained the most technically challenging surgery in the field of Cardio thoracic surgery. These surgical procedures have been associated with significant morbidity and mortality. They have always been the last domain to conquer for any Cardiothoracic surgeon.
In the early 20th century, the surgery for Aortic Aneurysm began with wrapping of the Aorta with cellophane tape and Ligation of the Aorta to prevent further aneurysmal dilatation of Aorta 2 .As expected these procedures, though heroic in those times, yielded poor results. Humanity had to wait at least for another 50 years for the invention of the Cardiopulmonary Bypass machine before any serious innovative surgical approaches to this disease could be contemplated. It took another couple of decades for Borst et al 1 to come up with the Elephant trunk operation which has stood the test of time and still remains the gold standard for treating aortic aneurysm/dissection involving the arch and DTA. Any advancements or innovations in this domain have been modifications of the surgical principle formulated by Borst.
The conventional Elephant Trunk (cET) procedure, while pioneering, necessitated a second stage surgery to complete the treatment. There is high risk of interval mortality during this waiting period for the second stage surgery 2 . In contrast, the introduction of the Frozen Elephant Trunk (FET) technique enables single-stage repairs and mitigates the risks associated with proximal endoleaks and stent migration, promoting distal aortic remodeling 2 . It necessitates the use of a preassembled or custom-made hybrid prosthesis 5 . The proximal portion is non-stented and consists of a Dacron sleeve for conventional surgical handling; the distal part consists of a stent graft 3 .
Our patient had chronic dissection flap in the arch of aorta extending into left subclavian artery and distally extending till the iliac bifurcation with extension upto the external iliac on the right and common iliac on the left. Initially debranching of the aortic arch followed by TEVAR was planned for him. As the patient had already undergone ascending aorta replacement and there was suspected kink in the old graft and also the dissection extending into arch vessels, Total Arch Replacement (TAR) was planned for him using FET technique as this will avoid second intervention.
The Thoraflex hybrid graft which we used in this patient, incorporates several design features aimed at optimizing its performance. The proximal part of the graft is particularly notable, featuring four arch branches arising from Gelweave woven polyester graft material. Three of these branches are dedicated to the three arch vessels, while the fourth serves as a branch for distal perfusion. This unique configuration simplifies the creation of anastomoses to the arch vessels and enables early perfusion to the distal part of the body after completion of the distal aortic anastomosis thereby reducing the risk of visceral ischemia and spinal cord injury. The proximal sewn graft and the distal anastomosis cuff of Thoraflex eliminates the risk of endoleak and stent migration.
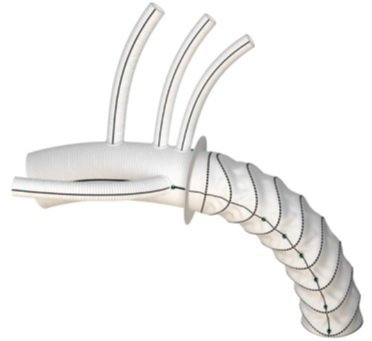
Fig. 6.
Thoraflex(TERUMO) hybrid graft used in this patient.
The Thoraflex hybrid graft offers versatility in its availability, with a wide range of diameters and options for stent lengths of either 10 cm or 15 cm. These options cater to the individualized needs of patients, ensuring a tailored approach to aortic surgery. The graft also includes gelatine impregnation, providing blood-tightness and reducing the risk of post-implantation complications.
The main surgical steps of FET include3
(i) total resection of the aortic arch;
(ii) preparation of the distal aortic stump with obliteration of the false lumen (FL) use of 4 or 5U stitches with pledgets inside and a Teflon felt outside;
(iii) advancement of the hybrid system in the descending thoracic aorta over a guidewire that has been retrogradely positioned via the femoral artery into the true lumen;
(iv) deployment of the stent graft;
(v) suturing of the vascular collar to the distal aorta before or after the origin of the left subclavian artery;
(vi) complete reimplantation of the arch vessels
(vii) completion of the proximal anastomosis
Selective Antegrade Cerebral Perfusion was used to decrease risk of ischemic injury to the brain during hypothermic circulatory arrest 4 This was established by cannulating the three arch vessels. Near Infrared Spectroscopy (NIRS) was used to monitor the oxygenation status of the brain during circulatory arrest. Also. to decrease the risk of spinal cord injury, CSF pressure was monitored and CSF drainage done if required.
As this patient had a narrow distal DTA beyond FET graft, distal DTA and Abdominal Aorta was addressed by TEVAR. The principal advantage of frozen elephant trunk is the potential to create a longer, more stable, and relatively kink-resistant proximal seal zone that facilitates planning and easier implantation of the distal endografts by TEVAR7. TEVAR following FET provides very good technical results however the risk of Spinal cord Injury and risk of endoleak is more. To prevent the risk of endoleak, it is important to maximize the overlap between the endograft components and the FET graft as has been done in this patient. This patient did not develop endoleak or Spinal Cord Injury (SCI) post procedure.
Conclusion
In this case report, we discuss about the management of chronic Aortic dissection which was complex because of an earlier surgery and involvement of the arch vessels. A Multi-disciplinary team including the CTVS surgeons, Cardiologist, Vascular Surgeons and Cardiac anaesthetists was deployed for the optimal management of this complex disease. Frozen Elephant Trunk operation using Thoraflex Hybrid( TERUMO) prosthesis was done for this patient. Followed by that, TEVAR using valiant captiva Medtronic device was done to address the diseased distal Descending Thoracic Aorta and Abdominal Aorta. This complex procedure resulted in symptom free patient and also addressed the risk of aortic aneurysmal rupture.
References
- Borst HG, et al. Extensive aortic replacement using “elephant trunk†prosthesis. Thor Card Surg. 1983;31(01):37-40.
- Hagl C, et al. Elephant trunks in aortic surgery: fresh and frozen. J Thor Card Surg. 2013;145(3):S98-102.
- Ruggero De Paulis, et al. Frozen versus conventional elephant trunk technique: application in clinical practice. Eur J Card Thor Surg. 2017;51(suppl_1):i20-8.
- Okita Y, et al. Surgical techniques of total arch replacement using selective antegrade cerebral perfusion. Ann Card Surg. 2013 Mar;2(2):222.
- Gambardella I, et al. Total arch replacement: Technical pearls. JTCVS techniques. 2021;10:8-13.
- Crawford ES, et al. Diffuse aneurysmal disease (chronic aortic dissection, Marfan, and mega aorta syndromes) and multiple aneurysm. Treatment by subtotal and total aortic replacement emphasizing the elephant trunk operation. Ann Surg. 1990;211(5):521.
- SVENSSON LG. Rationale and technique for replacement of the ascending aorta, arch, and distal aorta using a modified elephant trunk procedure. J Card Surg. 1992;7(4):301-12.

Dr. G. Anton Prem Thilak
Associate Consultant Cardio Thoracic Surgeon

Dr. Venkatesa Kumar Anakaputhur Rajan
Associate Consultant Cardio Thoracic Surgeon

Dr. P. Chandrasekar
Senior Consultant Anesthesiologist

Dr. Arunkumar Govindarajan
Senior Anesthesiologist

Dr. Sivakumaran Subbarayan
Cardio Thoracic Surgery

Dr. Harikrishnan Subramanian
Cardio Thoracic Surgery

Dr. Arani Raghavendrarao Raghuram
Senior Consultant, Cardio Thoracic Surgery

Dr. R. Anantharaman
Senior Consultant Interventional Cardiologist