Effectiveness of Rehabilitative approach-based management for Children with Japanese Encephalitis (JE)
Mahendran M 1, Bruno Raju 2, Ananth Kumar T3*
1Consultant Paediatric Occupational Therapist, HAMSA Rehab for kids, kauvery hospital Trichy
2Consultant physician, Department of PMR, HAMSA Rehabilitation Centre
3Senior.Physiotherapist, Department of physio Therapy, HAMSA Rehabilitation Centre, Kauvery hospital Trichy, Tamilnadu-620001
*Corresponding: therapy.trichy@hamsarehab.com
Abstract: The objective of study resources to explore the effect of Rehabilitative approach-basedinterventions on Children with aJapanese encephalitis (JE). Therefore, the focus of JE treatment is on symptom management, and thorough supportive care is crucial to prevent neurological sequelae. In this case study reported here, a Thirteen-year-old boy complained of loss of diminished tone, and fatalities. Management was planned using a rehabilitative approach that exclusively includes the use of evidence-based practice along with standard paediatric Occupational Therapy, Physical therapy, speech therapy protocol. Objectives created indicated that both preventing complications and facilitating recovery were important. The treatment protocol was provided for a period of eight weeks.
Methods: Prospective case study.
Results: The subject was composed with child sensory profile-2 score statistically significant differences were detected in all the studied variables (p 0.0009), between the pre-treatment and posttreatment results 8Weeks. In the 8 weeks, the changes were statistically extremely significant, functional independence score (level of functionality and participation of the patient’s upper and lower limbs) in the FIM Evaluation p 0. 0001. The greatest increase occurred in spontaneous play checklist use from pre assessment to post Assessment (p = 0.0002), reaching 88.87% active participation in bimanual play tasks. The quality of movement of the upper limb and lower limb a significant value due to the increase in active movements
p = 0.0183 and also reduced muscle tone changes were statistically extremely significant p = 0.001)
Conclusion: Effectiveness of Rehabilitative approach-based management for Children with Japanese Encephalitis (JE)
Keywords: Japanese encephalitis (JE), Occupational therapist, Physio therapy, Rehabilitative approach, protocol.
Background
The inflammation of brain tissue is recognized as Japanese encephalitis. It could ascend from a straightcontagion or determined a hematogenous pathway. Viruses’consistent herpes simplex, Japanese B encephalitis, mumps virus, etc. are usually responsible for encephalitis. Another indicator of JE is acute encephalitis syndrome. It should be renowned that JE only records for 1015% of incidences of AES, whose causes is typically unknown.Japanese encephalitis is one of the maximum common viral encephalitis types in the biosphere. Later, it was bare that the virus gone to the domesticFlaviviridae, a genus called after the prototype yellow infection virus (flava in Latin meaning yellow). In India, rashes of JE have been recognized in many locations subsequently 1955, creation it one of the furthermostthoughtful problems affecting children’s well-beingthrough case-fatality rates ranging from 0.360%. Deactivated mouse brain-derivative JE vaccine is available in contradiction of JE in India.Presently, the virus has a deep-rooted zoonotic broadcast cycle that contains pigs, aquatic natures and mosquitoes; human’s solitarygetssick by accident when bitten by an infected mosquito and perform as a dead-end host. Infection can be circumvented by limiting outdoor activity at nightly and dawn, wearing attires that reveal the minimum quantity of skin, getting the JE vaccine, and by means of mosquito disgusting.
The perseverance of rehabilitative approach uses to maximum level of independence and stabilize functional capacity. However, neurological sequelae can be seen in 3050% of clients with JE. Neurological sequelae like reformed consciousness, feebleness, hemiparesis, and quadriparesis), focal or generalized anomalous sensory (below registration and over registration), limb muscle tone (hypertonia and hypotonia), focal or generalized abnormal limb reflexes (hyperreflexia and hyporeflexia), analysis of recurringseizures, persistent extrapyramidal movement disorders were distinguished. Convulsions and high intracranial pressure are accomplished as part of the supportive care given to clients with JE.
The trunk and pelvic muscles are a part of the indispensable. Those muscles are enormouslyindispensable for conserving the stability of the spine and pelvis. To be precise, the muscles that framework the core are the front belly muscles, paraspinal muscles, back gluteal muscles that serve as the roof, hip girdle muscles, and pelvic girdle muscles that serve as the bottommostmusculature. Pelvic stability movements are compulsory to work the lower trunk and hip muscles alongside. The muscles aid in attainingprecise postures for the lumbar and pelvic areas by provision core stability.Occupational therapy assists in trunk muscle activities and physical therapy aid in trunk muscle movements, which results in healthy trunk muscular movement. Many occupational therapists use a multisensory therapy facilitate the adaptive responses or another special treatment tool to help patients with their balance and coordination. When the activities are executed on a sensory modulation and developmental level based, the trunk muscles may be activated more effectively as a patient’s posture is perturbed when a (multisensory) moves beneath them, and the muscles respond in order to help the patient maintain the ideal posture. Due to the clinical symptoms found in JE, there is an impairment in activities of daily living, which further affects the quality of life of the individual. So far, rehabilitation therapy has been beneficial.
Japanese Encephalitis (JE) Pathway and India Affected Districts State Wise
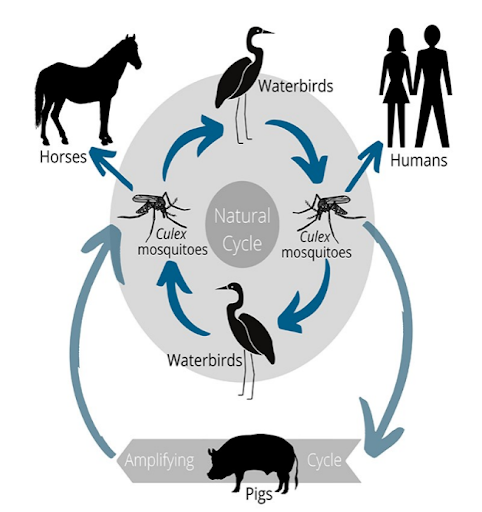
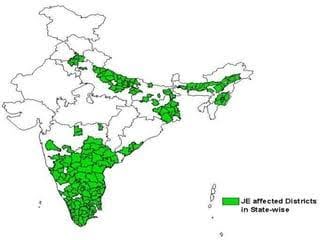
Source; indiabioscience.org
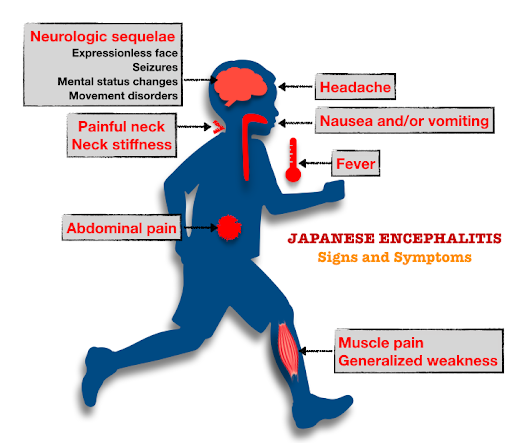
Source: Millennialpedia
Case Presentation
Patient information
Master, 13 years old male child was brought here in emergency department with complains of fever headache, vomiting for one day altered sensorium and 1episode of seizure. Onadmission, he had low GCS, tachypneia with hypertonia, exaggerated deep tendon reflexes. Acute meningo encephalitis with shock was clinically considered. Shock was resuscitatedwith IVfluids, and started on nor adrenaline infusion. In view of low GCS, he was intubated and connected to mechanical ventilator. IV fluids, IVAntibiotics, IVantiviral, anti-cerebral edema measures were started and was shifted to PICU for close monitoring.
Blood investigation showed thrombocytopenia with elevated CRP.Serum urea, creatininewas normal. Serum electrolytes was normal. Serum electrolytes were normal. Liver function test done showed elevated SGOT and SGPT. Other infective workup like Dengue and Scrub typhus were done. Doxycycline was added. Echo screening showed mild LV dysfunction. He was hemodynamically stable, inotroped was gradually tapered. He had marginal improvement in sensorium. CT brain done elsewhere showed diffuse cerebral edema. Neurologist opinion obtained and advised CSF analysis & MRI brain after stabilisation. MRI brain done showed multi T2/ Flair hyperintensities bilateral thalami basal ganglia, periventricular cortices and brain stem regions with significant blooming and diffusion restriction and without contrast enhancement-Viral encephalitis (JE). On day 4 of admission, he had recurrent seizure activity, IV Midazolam infusion was started. EEG done showed burst suppressed pattern. Fundus examination showed no evidence of papilloedema. Lumbar puncture was done, CSF analysis was done. CSF C and S was sterile. CSF JE 1gM antibody was positive.
There is no improvement in sensorium and he had difficulty in weaning off from ventilar. Tracheostomy was planned and done on 24.01.2023. Central venous catheterisation was secured in view of difficult peripheral venous access. Limb physiotherapy, Occupational therapy, swallowing therapy was started and continued. The nature, course of the disease and prognosis were clearly explained to the parents and was shifted to the ward. His tone gradually improved. Limb physiotherapy and paediatric occupational therapy was continued. Swallowing therapist was reviewed, Oro motor exercise was continued. He showed marginal improvement. Tracheostomy care, Suctioning Ryles tube feeding, Paediatric occupational therapy was (IEP) individual educational programme to the parents. His sensorium and swallowing capacity improved. He was discharged with KMC hospital to HAMSA PMR unit.
Methodology
This is a case study, before initiate the study, a knowledgeable consent form was given parent to the children family to participate, which definite the accurate to withdraw from the study at any time period, if mandatory by the participant. The inclusion criteria were a medical diagnosis of right Japanese encephalitis, age between 3 and 14 years, lack of activity of the affected upper limb and lower limb, bed mobility, adequate intellectual development to understand the non-verbal orders given for the execution of tasks and cooperation in their performance. In the same way, the exclusion criteria were visual problem that prevented the specific from delivery out the interference.
Treatment plan decided was to (FIM) functional independence measure scale evaluation pre and post intervention followed by rehabilitative approach therapy application, also along with extraction of retained primary play management followed by play checklist rating follow scale. Upper and lower extremity each major joints component should assess Muscle tone by Modified aswarth scale (MAS).Upper and lower extremity sensory component, General, Avoiding avoider, Sensory seeking, Registration by stander, component assess by sensory profile tool. Rage of motion component assesses pre and post. Developmental components by Denver scale. These scales component pre and post intervention statistically analysed.
Paediatric Occupational and physical Therapy assessment
Paediatric Occupational Therapy assessment based on detailed discussion with the parent and physical medical rehabilitation department head, the following goals were included in client therapeutic intervention program. Therapy was planned development level based with unstructured to structured activities and included Sensory Integration Therapy, Proprioceptive neuromuscular facilitation, Cognitive Perceptual training, activities of daily living skills and social emotional Training. His family members were invited to actively participate in sessions and Individual educational program was provided to his family on a regular basis to encourage continuity at home.
Physiotherapy he was admitted for rehabilitation with goals of training him in functional ambulation, independence in ADL’S and functional abilities, self-bowel and bladder management, on admission he had Hypotonia in B/L upper and lower extremities and poor hand grip was present, on examination upper and lower limbs muscle power-0, tone MAS-0 and sensory issues present, in physiotherapy he under went tone facilitation techniques for B/L upper and lower limbs, and passive range of motion exercise for both upper limb and lower limb, trunk and coremuscle strengthening exercise were given to improve his sitting and standing balance , techniques of self-transfers were taught and progressively he is getting good trunk and core muscle balances, at discharge he is independent in direct and pivot transfer from high plinth but need minimal support for low transfers, he was initially madeto stand within parallel bars followed by walking within the same. He progressed in his walking ability and progressed to stick walking and discharge he is able to walk independently with single stick.
The Occupational Therapy, Physical therapy intervention protocol
Problem identified |
Goal |
Treatment strategy |
Intervention |
| Hypotonia | To develop muscle tone in postural and phasic muscles | Facilitator’s techniques for roods approach//biomechanical FOR/sensory integrative approach | Cutaneous facillitation |
| Thermal facillitation | |||
| Proprioceptive facillitation | |||
| Inhibitory techniques | |||
| Lack of head and neck voluntary motor control | To enhance head and neck control | Facilitatory approaches and multisensory stimulation/spatial temporal adaptational approach/biomechanical FOR | Ontogenic motor patterns |
| assimilation | |||
| accommodation | |||
| Association, differentiation | |||
| Lack of pelvic, trunk control and efficient bed mobility | To enhance pelvic, trunk control and promote segmental bed mobility | NDT/PNF Approach//biomechanical FOR | Weight bearing-heavy/light |
| Bed mobility | |||
| Clasp hand with occupational therapy activities. | |||
| Trunk rotational activities | |||
| Scapula mobilization | |||
| Muscle strength techniques | |||
| Unilateral patterns | |||
| Bilateral patterns | |||
| Oro motor | a strength of grade | Oro-motor muscularfacilitation / Facilitator’s techniques for roods approach/sensory integrative approach | Oro-motor retraining |
| Tongue range of motion (ROM) exercises | |||
| Tongue thrust | |||
| Clock and anti-clock muscular facilitation |
Data Analysis and Results
The entire statistical test was performed using statistical package for graph pad instate software version 3.1 respectively.
Table 1: Characteristic of data pre- and post-evaluation Child Sensory profile (SP-2)
Characteristic of data-paired t-test |
pre-test evaluation (CSP-2) |
postpre-test evaluation (CSP-2) |
| Mean | 44.43 | 21.43 |
| standard deviation | 22.62 | 14.01 |
| Sample scale components | 14 | 14 |
| standard error (SE) means | 6.05 | 3.75 |
| 95% confidence interval difference | 11.31 | 34.69 |
Table 1; data shows pre and post (SP-2) test evaluation scores -scale components of subject, mean values are 44.43 and 21.43, respectively standard deviation 22.62 and 14.01 respectively sample components size 14, standard error of mean 6.05 and 3.75, the mean of pre and post 95% confidence interval of this difference 11.31 and 34.69, respectively.
Table 2: paired t’ test results between Pre and post of The Sensory profile-2 (SP-2) evaluation
S.No. |
Variable1 |
Variable2 |
Pvalue |
tvalue |
Level ofSignificance |
| 1 | Pre test | Post test | 0.0009 | 4.2493 |
statisticallySignificant |
Table 2: This shows that comparison between the pre-and post of The Sensory profile-2 (SP-2) in pre-evaluation test scores of subjects,t’ value is 4.2493 p-value is 0.0009 This difference is considered to be statistically significant.
Graph 1: Mean of Pre control and pre-post of evaluation -The Sensory profile-2 (SP-2)
Table 3: Characteristic of data pre-post evaluation-play checklist
Characteristic of data paired t-test |
(pre-test performance) |
(post-test performance) |
| Mean | 2.60 | 9.00 |
| standard deviation | 1.34 | 1.00 |
| Sample scale components size | 5 | 5 |
| The standard error (SE) means | 0.60 | 0.45 |
| 95% confidence interval | 7.82 | 4.98 |
Table 3; data shows of pre and post evaluation- of all -scale components of subject, mean values are 2.60 and 9.00, respectively standard deviation 1.34 and 1.00 respectively sample size 5, standard error of mean 0.60 and 0.45, 95% confidence interval 7.82 and 4.98, respectively.
Table 4: t’ test between characteristics of data pre-post evaluation-play checklist
S.No. |
Variable1 |
Variable2 |
Pvalue |
tvalue |
Level ofSignificance |
| 1 | pre-test evaluation | Post-test evaluation | 0.0002 | 12.5514 |
statisticallySignificant |
Table 4: This shows that comparison between the pre-post evaluation-play checklists (play-checklist) of all 01 subjects,t’ value is 12.5514 p-value is 0.0002, This difference is considered to be statistically significant.
Graph 2: Mean of data pre-post evaluation-play checklist
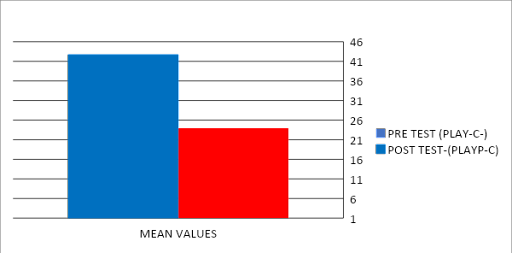
Table 5: Characteristic of data pre-post evaluation-Denver-2
Characteristic of data-paired t-test |
(pre-test evaluation) |
(Post-test evaluation) |
| Mean | 1.57 | 8.71 |
| standard deviation | 0.53 | 0.49 |
| Sample components size | 7 | 7 |
| The standard error (SE) means | 0.20 | 0.18 |
| 95% confidence interval difference | 7.97 | 6.31 |
Table 5 data shows thepre-post evaluation-Denver-2 -evaluation- scores of all -scale components subject, mean values are 1.57 and 8.71, respectively standard deviation 0.53and 0.49 respectively sample size 07, standard error of mean 0.20 and 0.18, 95% confidence interval 7.97 and 6.31 respectively.
Table 6: t’ test between pre-post evaluation-Denver-2
S.No. |
Variable1 |
Variable2 |
Pvalue |
tvalue |
Level ofSignificance |
| 1 | Pre-test evaluation | Post test evaluation | 0.0001 | 21.0042 | Extremely statistically Significant |
Table 6: Shows that comparison between the pre-post evaluation-Denver-2 – scores of all -scale components subjects, t’ value is 21.0042 p-value is 0.0001 This difference is considered to be statistically extremely significant.
Graph 3: Mean of the pre-post evaluation-Denver-2
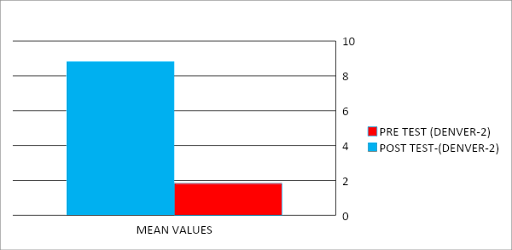
Table 7: Characteristic of data pre-post evaluation-FIM
Characteristic of data unpaired t-test |
Pre-test evaluation |
Post test evaluation |
| Mean | 1.00 | 5.83 |
| standard deviation | 0.00 | 0.38 |
| Sample scale components size | 18 | 18 |
| standard error (SE) means | 0.00 | 0.009 |
| 95% confidence interval difference | 5.02 | 4.64 |
Table 7 data shows data pre-post evaluation-FIM evaluation- scores of all -scale components subject, mean values are 1.00 and 5.83, respectively standard deviation 0.00 and 0.38 respectively sample size 18, standard error of mean 0.00 and 00.09, 95% confidence interval -5.02 and 4.64, respectively.
Table 8:t’ test betweenof data pre-post evaluation-FIM
S.No. |
Variable1 |
Variable2 |
Pvalue |
tvalue |
Level ofSignificance |
| 1 | Pre-test evaluation | Post test evaluation | 0.0001 | 53.4734 | Statistically Significant |
Table 8: This shows that comparison between data pre-post evaluation-FIM-evaluation- scores of all-scale components subject, t’ value is 53.4734 p-value is 0.0001 This difference is considered to be statistically significant.
Graph 4: Mean of data pre-post evaluation-FIM-evaluation
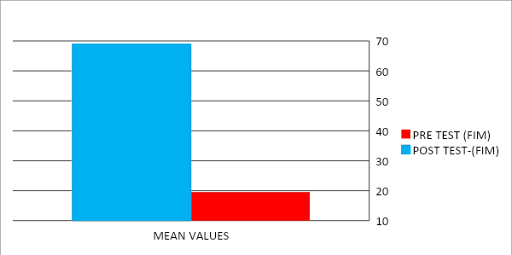
Table 9:t’ test between of data pre-post evaluation-ROM (Range of motion)
S.No. |
Variable1 |
Variable2 |
Pvalue |
tvalue |
Level ofSignificance |
| 1 | Pre-test evaluation | Post test evaluation | 0.0183 | 3.8517 | Statistically Significant |
Table 9: This shows that comparison between data pre-post evaluation-ROM-evaluation- scores of all -scale components subject, t’ value is 3.8517 p-value is 0.0183 This difference is considered to be statistically significant.
Graph 5: Mean of data pre-post evaluation-ROM-evaluation
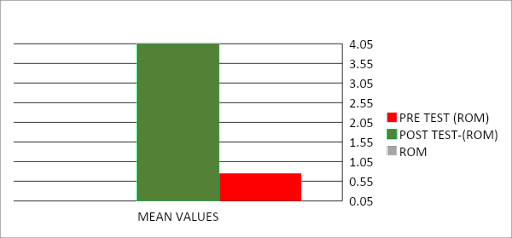
Table 10:t’ test between of data pre-post evaluation-MAS (Modified Aswarth scale)
S.No. |
Variable1 |
Variable2 |
Pvalue |
tvalue |
Level ofSignificance |
| 1 | Pre-test evaluation | Post test evaluation | 0.0001 | 20.1395 | Quit not Statistically Significant |
Table 10: This shows that comparison between data pre-post evaluation-MAS-evaluation- scores of all -scale components subject, t’ value is 20.1395 p-value is 0.0001 This difference is considered to be quit not statistically significant.
Graph 6: Mean of data pre-post evaluation-MAS-evaluation
Discussion
The overhead case study intends to demonstrate how effective rehabilitation can be providedwith the help of a Rehabilitation therapy to a persevering who has grieved from JE. This study’s outcomes are in line with those of anearlier study conducted by Kaleet al.; the duration of the Rehabilitationtherapy treatment was 8 weeks. Pre- and post-scores indicate that the master muscle tone and developmentalcondition, sensory componentshave improved. The key muscles of the UE and lower LE were considered. Both sides of each of the three muscle groups showed an improvement in muscle tone. According to the study, task-oriented therapy is very important for raising a child’s functional independencelevel. Theconsequences of this training are consistent with those ofKaleet al.’s training, in which the duration of the rehab therapy was 8 weeks. Promising results can be shown with obvious increases in muscle tone, stability, and mobility. The management of children task-directed therapy utilizing neurodevelopmental techniques (NDT), Sensory integration approach, Biomechanical FORRoods approach, and PNF has established to be productive.
Table 1; Table 1; data shows pre and post (SP-2) test evaluation scores -scale components of subject, mean values are 44.43 and 21.43, respectively standard deviation 22.62 and 14.01 respectively sample components size 14, standard error of mean 6.05 and 3.75, the mean of pre and post 95% confidence interval of this difference 11.31 and 34.69, respectively. Table 5 data shows there pre -post evaluation-Denver-2 -evaluation- scores of all -scale components subject, mean values are 1.57 and 8.71, respectively standard deviation 0.53and 0.49 respectively sample size 07, standard error of mean 0.20 and 0.18, 95% confidence interval 7.97 and 6.31 respectively. These results supported article Effect of core strengthening with pelvic proprioceptive neuromuscular facilitation on trunk, balance, gait, and function in chronic stroke. Sharma V, Kaur J.J Exerc Relabel.2017; 13:200205.
Table 5 data shows the pre-post evaluation-Denver-2 -evaluation- scores of all -scale components subject, mean values are 1.57 and 8.71, respectively standard deviation 0.53and 0.49 respectively sample size 07, standard error of mean 0.20 and 0.18, 95% confidence interval 7.97 and 6.31 respectively. This study supported results Effect of core strength on the measure of power in the extremities. Shinkle J, Nesser TW, Demchak TJ, McMannus DM.J Strength Cond Res.2012;26:373380.Table 7 data shows data pre-post evaluation-FIM evaluation- scores of all -scale components subject, mean values are 1.00 and 5.83, respectively standard deviation 0.00 and 0.38 respectively sample size 18, standard error of mean 0.00 and 00.09, 95% confidence interval -5.02 and 4.64, respectively. This article supported results and objectives byRehabilitation interventions in children and adults with infectious encephalitis: a systematic review protocol. Christie S, Chan V, Mollayeva T, Colantonio A.BMJ Open.2016; 6:0
Table 9: This shows that comparison between data pre-post evaluation-ROM-evaluation- scores of all -scale components subject, t’ value is 3.8517 p-value is 0.0183 This difference is considered to be statistically significant. Table 10: This shows that comparison between data pre-post evaluation-MAS-evaluation- scores of all -scale components subject, t’ value is 20.1395 p-value is 0.0001 This difference is considered to be quit not statistically significant. This Study Objective and Results Supported by Comparison of physio ball and plinth trunk exercises regimens on trunk control and functional balance in patients with acute stroke: a pilot randomized controlled trial. Karthik Babu S, Nayak A, Vijayakumar K, Misri Z, Suresh B, Ganesan S, Joshua AM.Clin Rehabil.2011; 25:709719.This study also supported results, benefit of early and goal directed physiotherapy intervention on gross motor function in a child with Japanese encephalitis: a rare case report. Kale R, Kovela RK, Qureshi MI, et al.J Pharm Res Int.2022; 36:40
The grades are also in mark with a preceding study, in which the authors examined the impact of activity configurational approach (ACA) and spatial playorientational therapy (SPOT) on functional ability and early learning accomplishment profile-based function in preschool-aged children with JE. In contrast to spatial playorientational therapy children with JE showed clear improvements UE,LE and gross motor function after receiving data-driven, functional ability therapy. The findings of the study create a crucial profile of patients with transferrable encephalitis in a rehabilitation background, which can help with better planning and provision of physical medical rehabilitation treatments.
In this case, when the master derived for physical medical rehabilitation on the first day, he was unable to move both the upper and left lower extremity, had a deficiency of neck and head control, lack of speech, and deglutition. But when we started the physical medical rehabilitation treatments, the main aim was focused on Ontogenic movement pattern, clasp hand activities, and Oro-motor muscular retraining to make the patient perform he activities daily living at simply, therebyration to improve the QOL of the patient. Additionally, the outcomes are consistent with the research where the activity configurational approach (ACA) and spatial playorientational therapy (SPOT) proved to be a useful tool for increasing trunk muscle motion, strengthening the core muscles of the trunk, maintaining stability in upright positions, and allowing freedom of movement for the upperextremity. As opposed to other adaptive device, the spatial playorientational therapy (SPOT) activities all weight-bearing kinds with lesschanges, needful less liveliness from the therapist. Compared to the outmoded therapy strategy, this method is more efficacy.
Conclusion
The effect of rehabilitative approach-based therapy showed better reducing in both the upper and left lower extremity muscle tone, increasing range of motion, Oro motor skills, posture, activities of daily living,sensory integrative among children with Japanese encephalitis (JE). There is a significant reducing in the functional difficulties of Japanese encephalitis child through active participation in rehabilitative approach-based treatment. From this case study can be concluded that in rehabilitative approach greater than individualized therapy,much more effective tool rehabilitation approach in bringing out changes in Japanese encephalitis children.
References
- Case report on encephalitis. Dhulse PS, Kurian B. J Pharm Res Int. 2021;33:645649.
- Efficient control of Japanese encephalitis virus in the central nervous system of infected pigs occurs in the absence of a pronounced inflammatory immune response. Redant V, Favoreel HW, Dallmeier K, Van Campe W, De Regge N. J Neuroinflammation. 2020;17:315]
- Viral diseases of the central nervous system. Swanson PA 2nd, McGavern DB. CurrOpinVirol. 2015;11:4454
- Clinical profile and outcome of Japanese encephalitis in children admitted with acute encephalitis syndrome. Kakoti G, Dutta P, Ram Das B, Borah J, Mahanta J. Biomed Res Int. 2013;2013:152656
- Japanese encephalitis. Solomon T, Dung NM, Kneen R, Gainsborough M, Vaughn DW, Khanh VT. J NeurolNeurosurg Psychiatry. 2000;68:405415
- Review of Japanese encephalitis vaccines in India. Chatterjee K, Bhadra A, Ray SK, et al. Asian Pac J Health Sci. 2022;9:272283
- Japanese encephalitis: a brief review on Indian perspectives. Kulkarni R, Sapkal GN, Kaushal H, Mourya DT. Open Virol J. 2018;12:121130
- Japanese encephalitis virus: ecology and epidemiology. Endy TP, Nisalak A. Curr Top Microbiol Immunol. 2002;267:1148
- Seizures and raised intracranial pressure in Vietnamese patients with Japanese encephalitis. Solomon T, Dung NM, Kneen R, et al. Brain. 2002;125:10841093
- Effect of core strengthening with pelvic proprioceptive neuromuscular facilitation on trunk, balance, gait, and function in chronic stroke. Sharma V, Kaur J. J Exerc Rehabil. 2017;13:200205
- Effect of core strength on the measure of power in the extremities. Shinkle J, Nesser TW, Demchak TJ, McMannus DM. J Strength Cond Res. 2012;26:373380
- Effect of pelvic control exercises on pelvic asymmetry and gait in stroke patients. Marzouk MH, El-Tamawy MS, Darwish MH, et al. Med J Cairo Univ. 2019;87:935939
- Trunk muscle activity during bridging exercises on and off a Swiss ball. Lehman GJ, Hoda W, Oliver S. ChiroprOsteopat. 2005;13:14
- Comparison of physio ball and plinth trunk exercises regimens on trunk control and functional balance in patients with acute stroke: a pilot randomized controlled trial. Karthikbabu S, Nayak A, Vijayakumar K, Misri Z, Suresh B, Ganesan S, Joshua AM. Clin Rehabil. 2011;25:709719
- Benefit of early and goal directed physiotherapy intervention on gross motor function in a child with Japanese encephalitis: a rare case report. Kale R, Kovela RK, Qureshi MI, et al. J Pharm Res Int. 2022;36:40]
- Gross motor function measure (GMFM-66 & GMFM 88) user’s manual 2nd edition clinics in developmental medicine edited by Dianne J Russell, Peter L Rosenbaum, Marilyn Wright, Lisa M Avery London, UK: Mac Keith Press, 2013 70.00 (spiral binding) pp 290 ISBN: 978-1-908316-88-2. Michaelis U. Dev Med Child Neurol. 2015;57:1188
- Goal directed physiotherapy treatment program for improving lower extremity function in a child with spastic paraplegic cerebral palsy. A case report. Krishna KR, Sinha MK. Indian J Public Health Res Dev. 2018;9:241244
- Activity focused and goal directed therapy for children with cerebral palsy–do goals make a difference? Löwing K, Bexelius A, Brogren Carlberg E. Disabil Rehabil. 2009;31:18081816
- Rehabilitation interventions in children and adults with infectious encephalitis: a systematic review protocol. Christie S, Chan V, Mollayeva T, Colantonio A. BMJ Open. 2016;6:0
- Swiss ball training to improve trunk control and balance in spastic hemiplegic cerebral palsy. Elanchezhian C, SwarnaKumari P. Sri Lanka J Child Health. 2019;48:300304

Dr. Mahendran M
Paediatric Occupational Therapist.

Dr. Bruno Raju
Consultant physician, Department of PMR

Dr. Ananth Kumar T
Senior Physiotherapist
Editorial
Editorial board
Cerebral Malaria: A case Report
Cefepime – Tazobactum – induced fluid – filled blisters (Bullous lesions): A case report
Blood Transfusion Reactions: An overview
Effectiveness of Rehabilitative approach-based management for Children with Japanese Encephalitis (JE)
The effect of nutritional composition on the Glycemic index and Glycemic load values
KCHs Pratidhi rises to the challenge: A triumph at the National QC Convention
Journal scan for the Clinical Pharmacist: A review of 10 recent papers of immediate clinical significance, harvested from the January 2024 edition of the MEDICINE, Elsevier
காவேரித்தாய் – 4
Nightingale – Volume 1 – Issue 1
Nightingale – Volume 1 – Issue 2
Nightingale – Volume 1 – Issue 3
Nightingale – Volume 1 – Issue 4
Nightingale – Volume 1 – Issue 5
Nightingale – Volume 1 – Issue 6
Nightingale – Volume 1 – Issue 7
Nightingale – Volume 1 – Issue 8
Nightingale – Volume 1 – Issue 9
Nightingale – Volume 1 – Issue 10
Nightingale – Volume 1 – Issue 11
Nightingale – Volume 1 – Issue 12
Nightingale – Volume 2 – Issue 1
Nightingale – Volume 2 – Issue 2
Nightingale – Volume 2 – Issue 3
Nightingale – Volume 2 – Issue 4
Nightingale – Volume 2 – Issue 5
Nightingale – Volume 2 – Issue 6
LOCATE US