Esthar Rani
Nursing Superintendent, Kauvery Heartcity, Trichy, India
*Correspondence: Tel No: +91 8508698000; estharrani@kauveryhospital.com
Nursing Care of a Patient with Coarctation of aorta (COA)
Abstract
Coarctation of aorta accounts for 5.8% of all congenital heart defects. Coarctation of the aorta may occur as an isolated defect or in association with various other lesions, most commonly bicuspid aortic valve and ventricular septal defect (VSD). Coarctation of aorta is a congenital (present at birth) heart defect involving a narrowing of the aorta. The aorta is the large artery that carriers oxygen rich (red) blood from the left ventricle to the body. The narrowed segment called coarctation of aorta.
Definition
Coarctation of aorta is a congenital (present at birth) heart defect involving a narrowing of the aorta. The aorta is the large artery that carriers oxygen rich (red) blood from the left ventricle to the body. The narrowed segment called coarctation of aorta
Background
Coarctation of aorta accounts for 5.8% of all congenital heart defects. Coarctation of the aorta may occur as an isolated defect or in association with various other lesions, most commonly bicuspid aortic valve and ventricular septal defect (VSD).
Case Presentation
A 9-year-old girl, known case of Discrete Coarctation of Aorta (severe), was admitted for Coarctation balloon dilatation.
Vitals: BP -140/80
Peripheral pulsations – Bounding at a rate of 110 bpm
ECG – within normal limits
Provisional Diagnosis:
Discrete Coarctation of Aorta (Severe)
Procedure in Cath Lab:
Right femoral artery and Left femoral artery access were obtained 2000IU Heparin was administered.
Baseline hemodynamics and aorta angiogram were obtained.
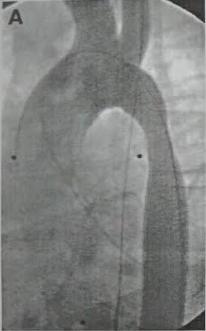


Measurements
Distal to proximal – 7.8 mm
Isthmus – 4.8 mm
Distal aorta – 904 mm
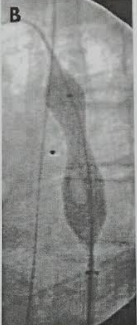
Isthmus was dilated with 10mm X 20mm mustang balloon with complete elimination of the wound.
Post dilation angiogram and hemodynmical were obtained
Sheaths were removed.
Good results as seen below:
Ascending Aorta
Descending Aorta
Pre Dilation
138/26
(104)
100/85
(96)
Post Dilation
129/78
(100)
120/78
(96)
ECHO
Post COA balloon dilatation, no significant residual gradient, good Bi- ventricular function (BVF), no effusion.
Discussion
Management of Coarctation of Aorta (COA):
Balloon angioplasty and stenting may be the first treatment for aortic coarctation.
Other options may have to be considered:
- Resection with end-to-end anastomosis
- Subclavian flap aortoplasty
- Bypass graft repair
- Patch aortoplasty
Balloon Angioplasty
This may be the first treatment for Aortic Coartation. Sometimes it is done if narrowing occurs again after Coartation surgery.
During balloon angioplasty the doctors inserts a thin, flexible tube, into an artery in the groin. It is moved through the blood vessels to the heart using X – Rays as a guide. An uninflected balloon is placed into the catheter and moved into the area of the narrowed aorta. The balloon is inflated.
The inflected balloon widens the Aorta so blood flows more easily.
Nursing Management
- Nurses maintained an hourly B.P chart. BP was stabilized.
- Nurses skilled in IV infusion and blood sampling techniques (Phlebotomy) obtained the samples for blood investigations like CBC, LFT & RFT with a sterile technique to prevent thrombophlebitis.
- Tagged the patient case note With NO CHEST PHYSIO mark.
- Diet was provided with salt – 5g/day, Fluid administer of 2 – 4 liter of water/day.
- Doctors explained the patient condition to the attenders. Nurses obtained consent for the clinical procedures after proper counseling.
- Keen observation & splinting for immobilization of femoral site was done to prevent complications.
- Nurses used AIDET technique (Acknowledge, Introduce, Duration, Explanation and Thank you) while communicating with patient and attenders to gain their confidence and improve the satisfaction level.
- Nurses monitored Femoral site for any active bleeding
- Maintained pulse chart with Doppler to prevent stasis and embolism formation. Vital parameters were keenly monitored during procedure and post operatively.
- Nurses cared for ADL activities, developed rapport with attender and patient which aids in early prognosis.
- Diversional therapy was provided with News papers, Television, Active listening to patient voice by Nurses.
Conclusion
Active listening to patient sufferings promotes the bonding and interpersonal relationship of nurses & patient thereby enhances good co-operation, quality of patient care.
After the interventional procedure, the patient became hemodynamically stable with efficient care of nurses.
Patient was discharged stable, and went home happily, with good prognosis.

Ms. Esthar Rani
Nursing Superintendent