Nursing challenges faced in care of patient with Blunt Injury Abdomen
Flora1,*, Jaya Menon2, Mahalakshmi3, Pradeepa4, Manju5, Anbarasi6
1Nursing Supervisor, Kauvery Hospital, Cantonment, Trichy, India
2Nursing Superintendent, Kauvery Hospital, Cantonment, Trichy, India
3Senior Staff Nurse, Kauvery Hospital, Cantonment, Trichy, India
4Staff Nurse, Kauvery Hospital, Cantonment, Trichy, India
5Staff Nurse, Kauvery Hospital, Cantonment, Trichy, India
6Staff Nurse, Kauvery Hospital, Cantonment, Trichy, India
*Correspondence: +91 75029 60512; flora.kcn@kauvery.in
Background
Abdominal trauma/injury caused by blunt force can be potentially fatal. A most common cause of blunt abdominal trauma is a road traffic accident. Violence is a close second. Blunt injury abdomen often leads to complications such as peritonitis, shock, bowel obstruction, abdominal aortic aneurysm, mesenteric artery tear etc.
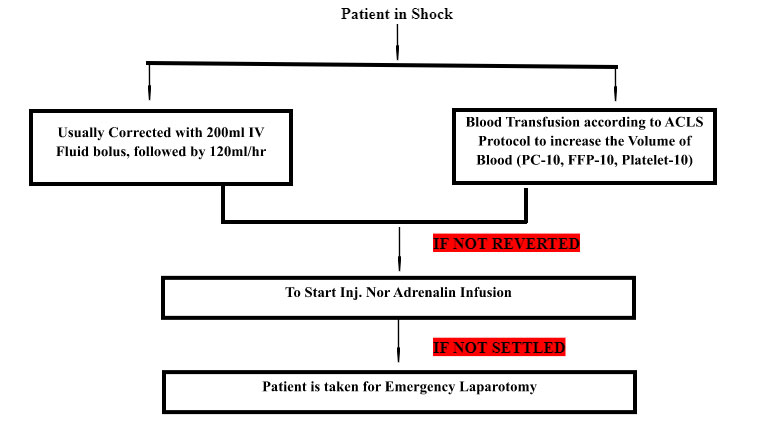
If in shock patient would present with hypotension, tachycardia and hypothermia, the “TRIAD” that portends serious trouble.
Clinical Pathway Management
Case Presentation
A 43Years old gentleman, with an alleged history of road traffic accident where he was hit by a 2-wheeler. The patient was received in ER with complaints of diffuse tenderness and guarding all over the abdomen.
Present History
History of RTA:
- Sustained injuries over abdomen and scalp region
- Diffuse abdominal pain since the injury
- One episode of vomiting
- Not passed flatus and stool
He was diagnosed as Blunt Injury to Abdomen
Past History
- No comorbidities
- No relevant past surgical history
On examination:
The patient was conscious, oriented and dehydrated
PR-138 beats/min, BP-80/60 mm/hg
CVS-S1, S2(+), RS-NV BS(+)
P/A – Distended, diffuse tenderness all over the abdomen. Guarding (+)
E-FAST examination findings (Extended Focused Assessment with Sonography, in Trauma):
CECT Abdomen and Pelvis examination: Bowel injury with peritonitis due to perforation
Ultrasound Abdomen: Fatty Liver
Procedure Done
Laparotomy and primary closure of perforation plus exteriorization of resected bowel end, under GA.
Post-operative events:
- Intubation done and patient connected to ventilator in SIMV mode.
- Continuous infusion of sedation
- Administration of Total Parenteral Nutrition (TPN)
- Comprehensive coverage was given by Intensivist and Cardiologist (for early extubation),Hematologist (for low platelet counts:-9000), Endocrinologist (for persistent hypoglycemia) and Microbiologist (for culture reports and advice on best antibiotic of choice)
- As patient may need prolonged ventilation and ICU care, tracheostomy was done on 4th OPD.
- Antibiotics were given per the culture and sensitivity report
- On the 14th post-operative day, weaning was done from ventilator, started on BIPAP and O2 support and shifted to the ward.
- Oxygen support was slowly tapered and decannulation of tracheostomy was done on the 32nd postoperative day.
- The patient was discharged to home 36th day with advice on medications and review date.
Nursing Care
Prevention of VAP (ventilator-associated pneumonia)
The patient was on mechanical ventilation for 14 days. Adherence to the bundle care list helped to prevent VAP.
Prevention of CLABSI (central line associated blood stream infection)
- Central Line was needed for the administration of higher-end Antibiotics and TPN.
- A low Platelet count (Nearly 9,00) was corrected with Platelet transfusion
- Central Line maintained more than 14 days without CLABSI, achieved with Bundle Care.
Prevention of CAUTI (catheter associated urinary tract infection)
- The patient was on continuous bladder drainage throughout admission till discharge for about 35days
- CAUTI care bundle was followed to prevent Catheter-Associated Urinary tract Infection.
Maintenance of Skin Integrity
Followed all measures to prevent pressure injury and related injury with proper guidance of the Tissue Viability Team
- Risk Assessment was done using Braden Scale in each Shift
- Turn-O-Clock position chart followed for 2nd Hourly Position Changing
- Back Care was given every 4th Hourly
- The surface of the bed was changed by using foam wedges, pillows and airbed to relieve constant pressure over the pressure points.
- Skin moisture maintained neutrally
- Dehydration prevented and balanced nutrients provided according to dietician’s assessment
Prevention of DVT
- The patient was provided with DVT (deep venous thrombosis) prophylaxis (Inj. clexane, DVT Pump and DVT Stockings)
- Early mobilization and limb physiotherapy were encouraged based on the patient’s condition
Conclusion
The nurses play the primary role and responsibility in providing care as well as monitoring patients during their hospital stay. They play the most important role in delivering patient education. For patients with minor blunt trauma, the outcomes are good but for those who suffer multiple organ injuries, the in-hospital mortality can vary from 3-10%.
There is a key need for educating the public on the need to avoid distractions while driving like eating, texting or using a mobile phone, to wear a safety belt, and be educated about defensive driving by maintaining a safe distance from other automobiles on the road.

Ms.Flora
Nursing Supervisor