Pituitary Macroadenoma: A case report
Sahayaselvi1,*, Aarthi2
1ANS Kauvery Hospital, Tennur
2Staff Nurse, Kauvery Hospital, Tennur
*Correspondence: maha@kauveryhospital.com
Background
The pituitary gland is also called the master gland of the endocrine systembecause it controls the functions of many of the other endocrine glands. The main function of the pituitary gland is to produce and release several hormones that help carry out important bodily functions
Pituitary adenomas are benign tumours of the anterior pituitary gland. They’re non-cancerous but they can interfere with normal pituitary function and cause certain health conditions. About 77 out of 100,000 people have a pituitary adenoma but researchers think adenomas actually occur in as many as 20% of people at some point in their lives. Healthcare providers treat pituitary adenomas with surgery, medication, radiation or a combination of these therapies.
Case Presentation
A 57-years female was admitted with headache and seizure. H/o headache for three years, and one episode of seizure for one month. Patient was known to have DM and HTN. She also had history of hypothermia couple of times in the last 2 years. She had undergone ureteroscopic lithotripsy (URSL) in the recent past for ureteric calculus.
On examination, the patient was conscious and oriented, GCS-E4V5M6, Moving all limbs PR: 86 b/min, BP: 110/70 mm Hg, RR: 20/min, SpO2: 97% in room air.
MRI scan reported Pituitary Gland enlargement; craniocaudal dimension (1.1 cm). On evaluation, patient was found have the lesion in the sellar region. Intrinsic T2 hyper and T1 hypo-intense areas were seen with FLAIR hyper intensities. Homogeneous post contrast enhancement of the pituitary gland.
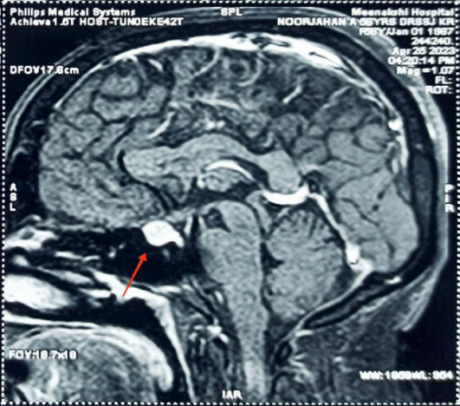
Fig 1. MRI brain Pituitary gland enlargement measuring 1.1 cm noted.
Hormonal evaluation and field of vision evaluation were done and it was found to be normal. Opinion was obtained from cardiologist anesthetist for fitness of surgery.
Endocrinologist and ENT opinion was obtained for Endoscopic trans-nasal trans-sphenoidal resection of the pituitary tumor. Patient was taken for trans-nasal trans-sphenoidal excision of pituitary adenoma on 16.05.2023.
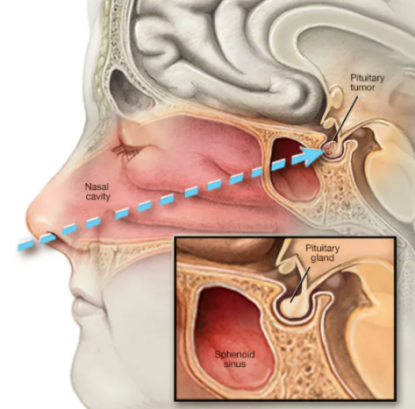
Fig. 2.Endoscopic transnasal transsphenoidal surgery – a surgical instrument is placed through the nostril and alongside the nasal septum to access the pituitary tumour
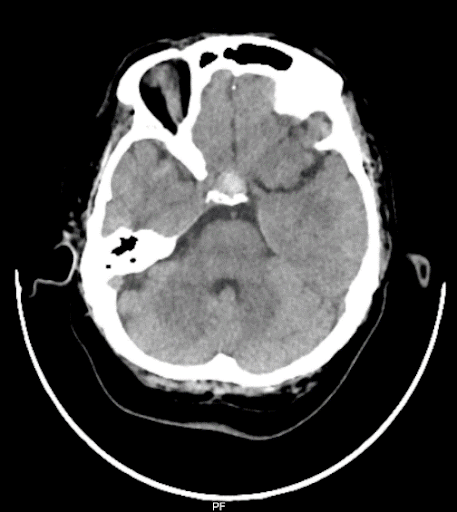
Fig. 3. Post-op CT brain Postoperative changes with areas of hemorrhage in the pituitary fossa.
Surgical Management for Trans-sphenoidal pituitary
Nursing care for patients with pituitary disorder includesassessment, patient education, evaluation of patient response, and providing support. A complete history and physical examination are performed to detect specific clinical findings.
Nurses must make sure the patient has free access to oral fluid and carefully monitorurine output, urine-specific gravity, urine osmolality, serum sodium level, serum osmolality and mental status.
Pressure on face/exertion:
- Advised to avoid direct firm pressure on the face for at least 4 weeks.
- Nose blowing or sneezing with mouth closed should be avoided for at least 12 weeks after surgery.
- Try to sneeze with mouth open for 12 weeks to avoid generating high pressure in your head.
Monitoring Neurosurgical Complications
- The nurses performed the neurological assessment
- Trans-sphenoidal (TS) surgery approaches a tumor that sits below and often compresses the optic nerves. So nurses checked the visual acuity, visual fields and extraocular movements every hour in the first 24 hours post Trans-sphenoidal (TS) surgery.
- Nurses monitored closely and teach the patient to report any excessive clear fluid drainage from the nose, particularly when the patient bends over as this may represent CSF rhinorrhea.
Fluid Maintenance
- Assessed and evaluated the patient skin color and turgor, mental status and body temperature.
- Monitored and recognized evidence of fluid and electrolyte imbalances such as nausea and vomiting and body weakness.
- Monitored intake and output closely. Recognized signs of fluid imbalances.
Diet Education
- Frequent small meals (4-6 per day) are suggested with a moderate amount of protein in each to assist in the healing process.
- Advised to avoid straining hard for bowel movements for 3 months.
- Advised to take plenty of fluids and fiber (fruits vegetables) diet.
Health Education
Work:We advised the patient to be plan for 2-4 weeks if they have a sedentary job and 6 weeks if they have an active job.
Lifting weights: Advised specific limitations on weight lifting, swimming and any other activity involving great physical exertion.
Sleeping
- Advised the patient to elevated the head on pillows may help decrease headaches.
- Keep it elevated at least 30 degrees for 10 days after surgery
- After surgery you may be placed on Prednisone or Dexamethasone. It is important to continue to take this medication daily until instructed to stop and endocrinologist will monitor sodium and hormone levels in the weeks after surgery.
On 7th POD
She was ambulated, no C/O head ache, bleeding CSF rhinorrhoea. catheter was removed voided freely. Her postoperative period was uneventful. Regular ENT follow up was done.Now as condition of the patient was stable and she wasdischarged with the following advice.
Tab. Brevipil, 100mg 1-0-1 x 2 weeks
Tab. Pyrigesic, 1gm 1-1-1 x 5days
Tab. Diamox 0-0-1 x 2 weeks
Tab. Pantocid 1-0-1 x 2 weeks
Tab. Creamaffin10ml 1-1-1 x 5 days
Lacto brain sachet 1-0-0 x 2 weeks
Conclusion
The prognosis of pituitary adenomas depends on its being functioning or non-functioning.The non-functioning adenomas and prolactinomas have an excellent prognosis if treated promptly with surgery or medical therapy. Nurses are responsible for recognizing patient’s symptoms, strictly monitor the positions, taking measures within their scope of practice to administer medications, monitor nasal bleeding and CSF leakage and providing other measures for symptom alleviation and collaborating with other professionals to optimize patients comfort and families understanding and adaptation. The patient condition was stable anddischarged.

Ms. Sahayaselvi
Assistant Nursing Superintendent

Ms. Aarthi
Staff Nurse