Postpartum/Peripartum Cardiomyopathy
Mercy1,*, S Pradeepa2, Roja Jency3
1Critical Ward Incharge, Kauvery Heartcity, Trichy, India
2Staff Nurse, Kauvery Heartcity, Trichy, India
3Staff Nurse, Kauvery Heartcity, Trichy, India
*Correspondence: Tel: +91 8508698000; email: nursing.heartcity@kauveryhospital.com
Background
Postpartum or peripartum Cardiomyopathy (PPCM) is a rare form of congestive heart failure of unknown etiology. Heart failure in the Peripartum period was first described in 1849. The current diagnostic criteria for Peripartum Cardiomyopathy include:
- Cardiac failure in a previously healthy woman in the last month of pregnancy or within 5 months of delivery.
- Absence of a determinable etiology for the cardiac failure.
- Absence of demonstrable cardiac disease prior to the last month of pregnancy.
- Echocardiographic evidence of diminished left ventricular systolic function.
- Its incidence and prevalence are highly variable depending on the race and geographic regions.
- Its clinical outcome is also diverse from complete recovery to death.
Post partum cardiomyopathy is a diagnosis of exclusion.
Case Presentation
A 26 years old female, G3 P3 L3, came to the casualty with complaints of breathing difficulty and chest burning sensation since 1 week. Patient was initially treated at an outside hospital and came to Heartcity for further management and got admitted on 07.09.2022.
Chief Complaints
- Feeling of heart racing or skipping beats (palpitations).
- Shortness of breath with activity and when lying flat Fatigue.
- Increased night time urination.
- Swollen ankles.
- Swollen neck veins.
- Giddiness and weakness on standing up.
Past History
Patient had a normal vaginal delivery 75 days back.
- L1 Male (6 years)
- L2 Female (4years)
- L3 Female 75 days
Previous pregnancies were normal
Examination
- CVS: HR – 130 /min, S1 S2+, BP – 50/? mmHg
- RR – 32/mt, RS: B/L crepts +. SAO2 – 90 RA ,
- Temp – Normal
- P/A: Soft
- CNS: NFND
- GCS – 15/15
- GRBS – 109 mg/dl
ECG:
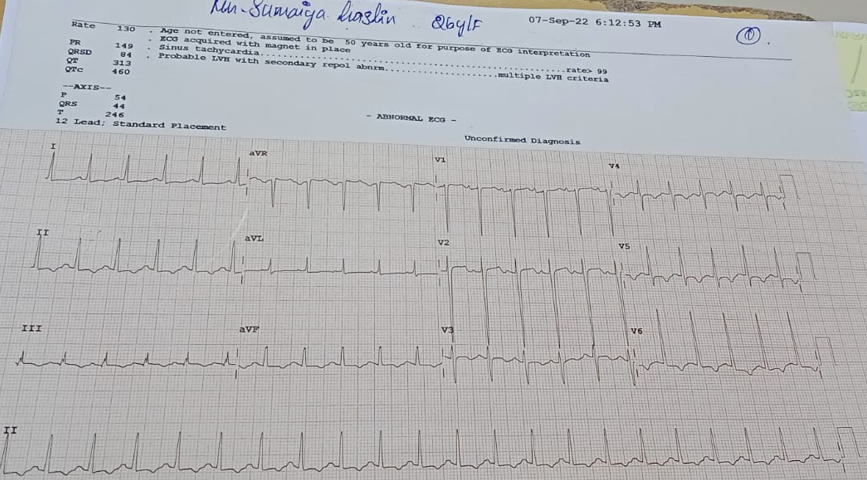
Tachycardia, Inferior and Lateral wall T inversion
Lab Report: Nil significant. COVID RT-PCR – Negative
ECHO: Dilated LA and LV, Global Hypokinesia of LV, Grade II Diastolic dysfunction, Moderate MR,Moderate PH, Mild TR, moderate RV dysfunction, IVC dilated
Chest X-Ray: Cardiomegaly, hilar vessels prominent

Medication
Tab. Ivabrad 5mg PO BD 1-0-1
Tab. Aldactone 25mg PO BD 1-0-1
Tab. Lanoxin 0.25mg OD 1/2-0-0
Inj. Heparin 5000 BD 1-0-1
Inj. Xone 1gm IV BD 1-0-1
Discussion
Peripartum Cardiomyopathy, also known as Postpartum Cardiomyopathy, is an uncommon form of heart failure that happens during the last month of pregnancy or upto five months after giving birth. Cardiomyopathy literally means heart muscle disease.
Etiology
The exact mechanism of the disease is unknown; however different hypotheses have been described regarding its etiology comprising of viral myocarditis, nutritional deficiencies, autoimmunity, hemodynamic stresses, vascular dysfunction, hormonal insults and underlying genetics.
Most patients present soon after delivery especially in the first week postpartum. The symptoms are suggestive of heart failure, for example, orthopnea and paroxysmal nocturnal dyspnea. These symptoms are usually attributed to normal pregnancy and that is why a diagnosis of peripartum cardiomyopathy can be easily missed.
Physical examination findings include tachycardia, elevated jugular venous pressure, bilateral pulmonary crackles due to pulmonary edema, third heart sound (S3) and displaced apical impulse.
Severe cases may present with acute respiratory failure or cardiogenic shock and often need close monitoring in the intensive care unit.
Some of the most common risk factors for the development of postpartum cardiomyopathy are as follows:
- Advanced maternal age (more cases reported in both extremes of age).
- High parity (71% of women diagnosed with PPCM had three or more prior pregnancies.
- High gravidity.
- Twin pregnancy (more endemic in women with twin pregnancies).
- Use of Tocolytic therapy (Greater than 4 weeks can cause silent ischemia).
- African descent (more prevalent in the African population).
- Poverty.
- Hypertension.
- Cocaine abuse
Nursing Management
Drugs are the primary treatment, and include an ACE Inhibitor or ab AR Blocker, a cardio selective betablocker, a diuretic that is an Aldosterone inhibitor like Spironolactone and anticoagulation when severe LV dysfunction is present as there is a high risk of forming an LV thrombus and systemic embolization
Management in the coronary care unit or intensive care unit is usually required due to the severity of the condition. This opens up possibilities for even more interventions not just pharmacological but also hemodynamic monitoring and cardiovascular supportive therapy such as ventricular assist devices.
Common nursing interventions followed were:
- Daily bedside care and assisting the patient in his activities of daily living
- Administration of medication regularly
- Postpartum care
- Assisting the patient in breastfeeding the baby.
- Monitoring of vitals and recovery progress regularly
Patients need long term monitoring of their cardiac status and adherence to treatment.
Most importantly, a subsequent pregnancy is not advised unless an EF of 60 % or above is achieved and maintained
Recovery
After a stay of 4 days in the hospital, patient became stable with the efficient care of nurses and went home happily with good prognosis.
Condition at Discharge
- General Condition: Patient conscious and oriented.
- Vital Signs: PR: 92bpm, BP: 100 /60 mmHg
- CVS: S1 S2 (+)
- RS: BAE (+)
- P/A: Soft
- CNS: Within normal limits
Discharge Medication
| TAB.CEFTUM | 250MG | 1-0-1 X 5 DAYS |
| TAB.DYTOR | 10MG | 1-0-0 |
| TAB.CARDACE | 1.25MG | 0-0-1 |
| TAB.IVABRAD | 5MG | 1-0-1 |
| TAB.ALDACTONE | 25MG | 0-1-0 |
| TAB.DOLO | 650MG | SOS |

Mercy
Critical Ward Incharge, Kauvery Heartcity

S. Pradeepa
Staff Nurse, Kauvery Heartcity

Roja Jency
Staff Nurse, Kauvery Heartcity