J Jane Abishak1,*, A. Mercy2, K. Priyadharshini3, Akshaya4
1CCU Supervisor, Kauvery Heartcity, Trichy, India
2CCU Incharge, Kauvery Heartcity, Trichy, India
3CCU Senior Staff Nurse, Kauvery Heartcity, Trichy, India
4CCU Staff Nurse, Kauvery Heartcity, Trichy, India
*Correspondence:Tel: +91 8508698000; E-mail: nursing.heartcity@kauveryhospital.com
Background
Pulmonary Thromboembolism is a condition in which one or more arteries in the lungs get blocked by a blood clot. Most times a pulmonary embolism is caused by blood clots that travel from the veins of the legs or rarely from other veins, a condition termed as Deep Vein Thrombosis (DVT). Leg pain or swelling may occur due to DVT, but there may be no symptoms. The most common symptoms of pulmonary thromboembolism include shortness of breath, chest pain, and cough. DVT is detected through Duplex ultrasonography, which is an imaging test that uses sound waves to look at the flow of blood in the veins. Common treatment includes thrombolytics and anticoagulants. Prevention includes the use of compression stockings.
Case Presentation
A 44 years old female patient came with the complaint of difficulty in breathing for 2 days and chest pain on and off.
Past History
She had a history of Type II DM for 3 years and systemic hypertension for 7 years. Also, the patient had irregular treatment for Pulmonary Thromboembolism & and Deep Vein Thrombosis in 2017.
On Examination
SpO2: 88 at room air-pulse: 100/mt, BP: 180/50mm Hg-RR: 29/mt
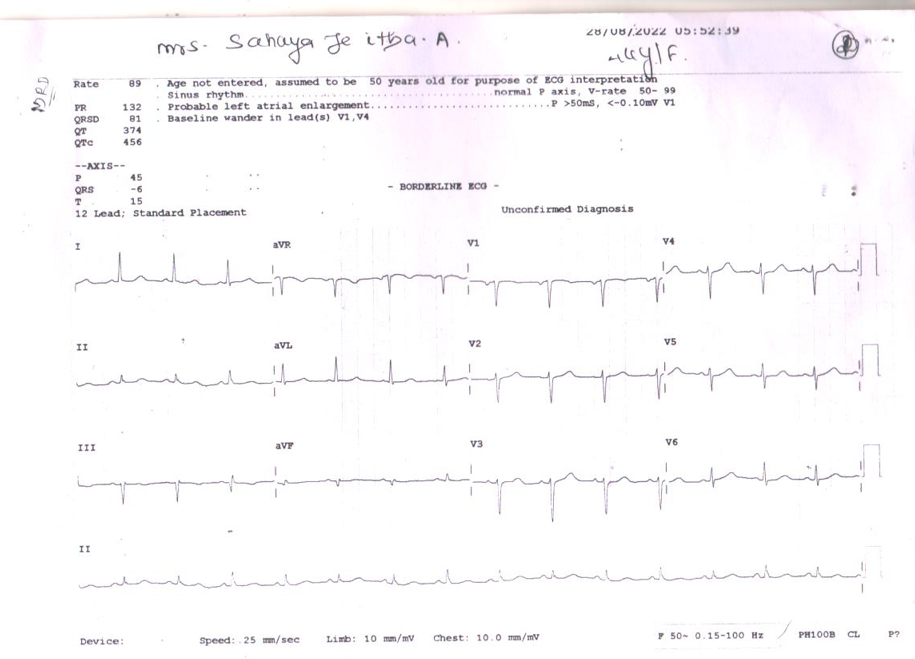
ECG
Unremarkable except for the dominance of S waves in the precordial leads
ECHO Findings
Good LV function, grade I diastolic dysfunction, Aortic sclerosis, moderate TR, PAH, Mild concentric LVH
USG Findings
Hepatomegaly grade I, fatty liver, bilateral lower limb Doppler.
D Dimer is not done.
CT Angiogram Findings
CT pulmonary angiogram revealed acute pulmonary thromboembolism involving segmental arteries of the right upper and bilateral lower lobes with ground glass densities in bilateral lung fields.
Diagnosis
Severe PAH, RA RV dilated,? Pulmonary Thromboembolism, Type II DM, SHTN.
On Admission Treatment
Inj. Streptokinase 1 lakh/hr started on 27.08.2022 at 09:00 pm to 29.08.2022 at 06:00 am (33 Hrsh).
Inj. Heparin 5000U as IV of Q6H 2 days administered as per doctor’s advice.
Tab. Ivabradine 5 mg BD.
Nursing Care
- Maintained interpersonal relationships with the patient and family members.
- Patient The patient was assessed with the skin integrity on a daily basisdaily to prevent dehydration, skin tear, and pressure points for bedsores.
- Necessary investigations were done on a daily basisdaily to monitor his health improvement.
- The assigned nurses communicated with the patient reassuring him about his health status and gave giving him orientation to time place and person.
- Nurses co-ordinate with other health care professionals for care while doing X-Ray, arranging diet at the appropriate time, and for other timely investigations.
- Nurses positioned him two hourly2 h round the clock and provided back care and back massages like effleurage, petrissage, tapping, and friction, for prevention of bed sore. Each nurse communicated effectively and developed a good rapport with the patient and attender and he cooperated well in his care.
- Inj. Heparin was administered by the staff nurse as per the doctor’s advice is 5000U as IV of Q6H.
- Nurses developed a home home-like environment for him to relax and encouraged him to sit on the chair with O2 support every day.
- Opinions were obtained from Nephrologists and orders were carried out respectively.
- Adequate hydration was maintained with oral liquids and IV fluids.
- Advised the patient not to take cool drinks, over fluids, and frozen items.
Discharge Condition
General condition: Patient conscious and oriented.
Vital Signs: PR: 94 bpm, BP: 140/90 mmHg, SpO2: 96%, RR: 20 p/m, CVS: S1 S2 (+), RS: BAE (+), P/A: Soft, CNS: Within normal limits Advice on Discharge
Diet
1500 Kcal low-fat, salt-restricted and diabetic diet.
Discharge Medications
<td”>
Inj Human MIXTARD 30/70
| Eliquis (anticoagulant) | 10 mg | 1-0-1 × 1 Weekweek |
| Thereafter Eliquis | 5 mg | 1-0-1 |
| Tab. Ivabradine | 5 MG | 1-0-1 |
| DM advice: | ||
| Inj Human Actrapid | S/C | 14U-14U-0 |
| S/C | 0-0-16U |
Conclusion
After a long stay in the hospital, the patient became stable with the efficient care of nurses and got discharged.

J. Jane Abishak
Critical Ward Supervisor, Kauvery Heartcity

A. Mercy
Critical Ward Incharge, Kauvery Heartcity

K. Priyadharshini
Critical Ward Senior Staff Nurse, Kauvery Heartcity

Akshaya
Critical Ward Staff Nurse, Kauvery Heartcity
</td”>