L. Indumathi
Nurse Educator, Kauvery Hospital, Salem, India
*Correspondence: Tel: +91 96260 55335; email: indumaya1986@gmail.com
Wireless moonlight: An ultra-short case study
Case Presentation
A 70 years old gentleman who had chest pain on 26-06-2022 was taken to outside hospital for treatment and he was referred to Kauvery hospital, Salem for further management.
He presented to emergency department on 01.07.2022 at 4.18 pm with the history of chest pain and palpitation for the past 1 month but aggravated from afternoon. There was no history of dyspnea, cough or pain radiating to neck.
Patient was a known case of Parkinsonism for past 18 years and on regular drugs for the same. He was not known to have comorbidities like Hypertension/Diabetes Mellitus.
Vital signs on admission
Heart rate: 22 beats/min; Respiration: 20 breath/min; blood pressure: 100/60 mmhg; Spo2 – 97%; Weight- 60 kg; CBG -175 mg/dl
ECG findings: Severe bradycardia due to absence of Atrial Ventricular conduction, Atrial Ventricular dissociation with independent Atrial and ventricular rate. So patient was diagnosed as Complete Heart Block.
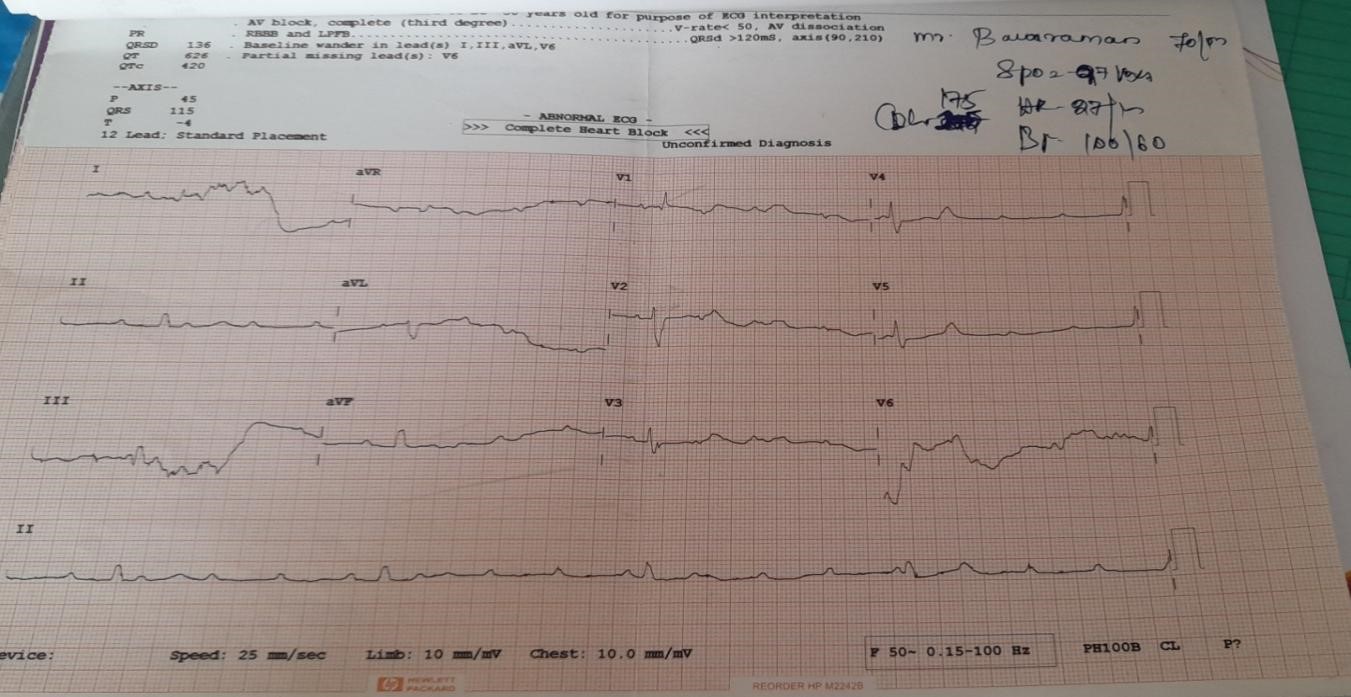 Fig. 1: ECG on admission – Bradycardia HR- 22 beats/min. the P waves are not related to the QRS complexes; patient diagnosed as complete heart block.
Fig. 1: ECG on admission – Bradycardia HR- 22 beats/min. the P waves are not related to the QRS complexes; patient diagnosed as complete heart block.
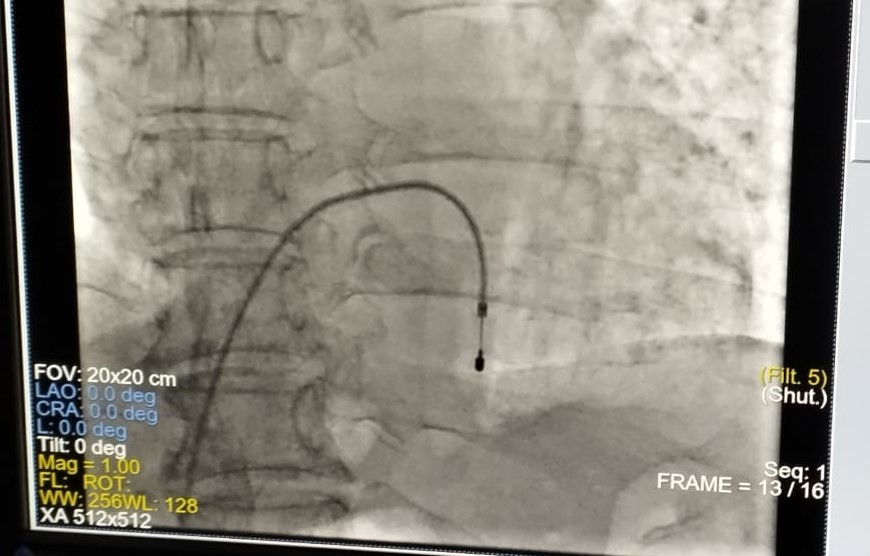 Fig. 2: Temporary pacemaker insertion procedure done on 01-07-2022. Right femoral vein approach; temporary lead inserted and fixed at RV apex. Set rate-80 beats/min.
Fig. 2: Temporary pacemaker insertion procedure done on 01-07-2022. Right femoral vein approach; temporary lead inserted and fixed at RV apex. Set rate-80 beats/min.
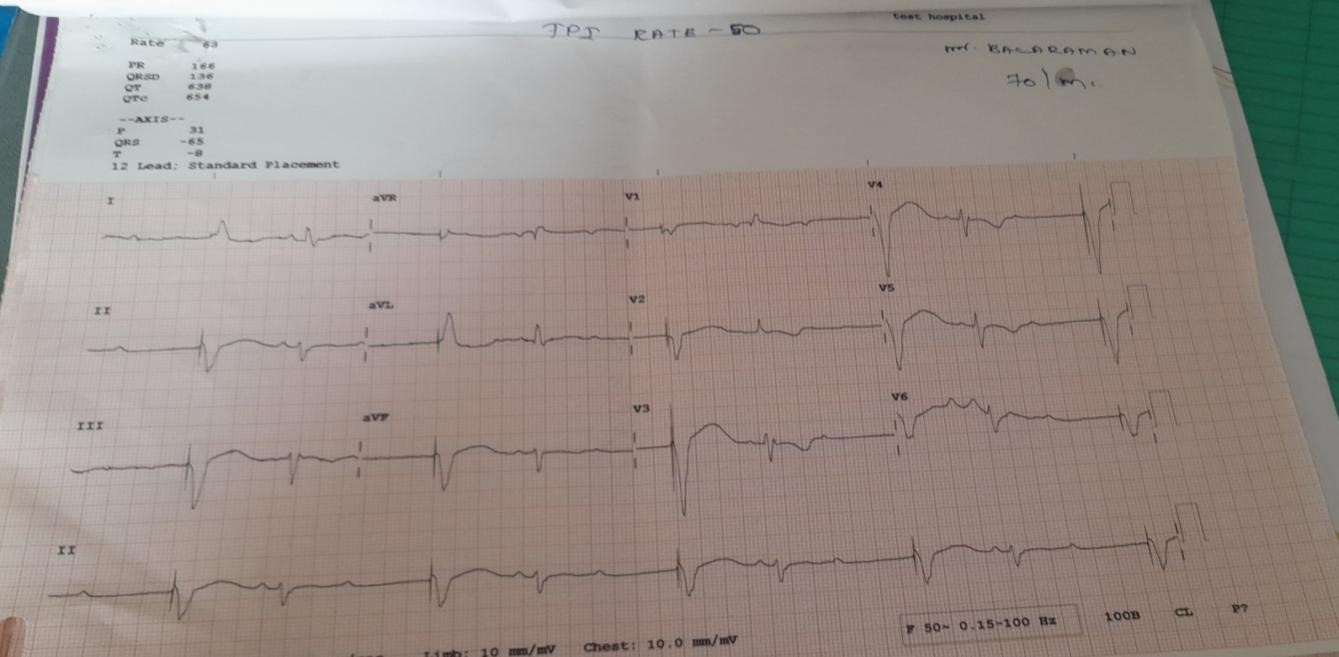 Fig. 3. ECG taken post TPI insertion; Heart Rate was 50 beats/min.
Fig. 3. ECG taken post TPI insertion; Heart Rate was 50 beats/min.
As the patient was in continuous bradycardia of HR – 48b/min. So he was planned for Permanent pacemaker insertion (PPI).
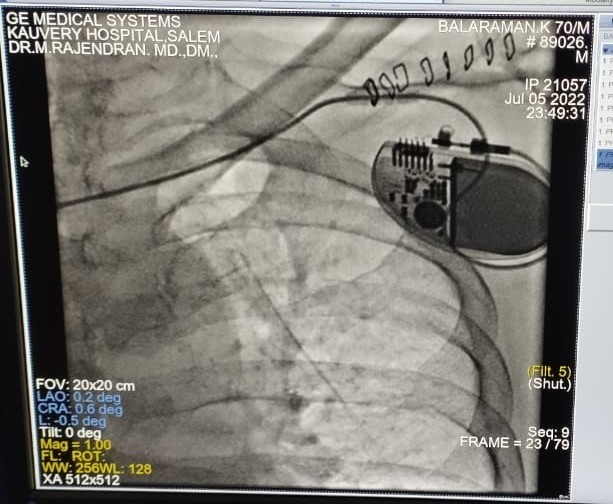 Fig. 4. Permanent Pace Maker insertion with VVI Mode is shown in the picture.
Fig. 4. Permanent Pace Maker insertion with VVI Mode is shown in the picture.
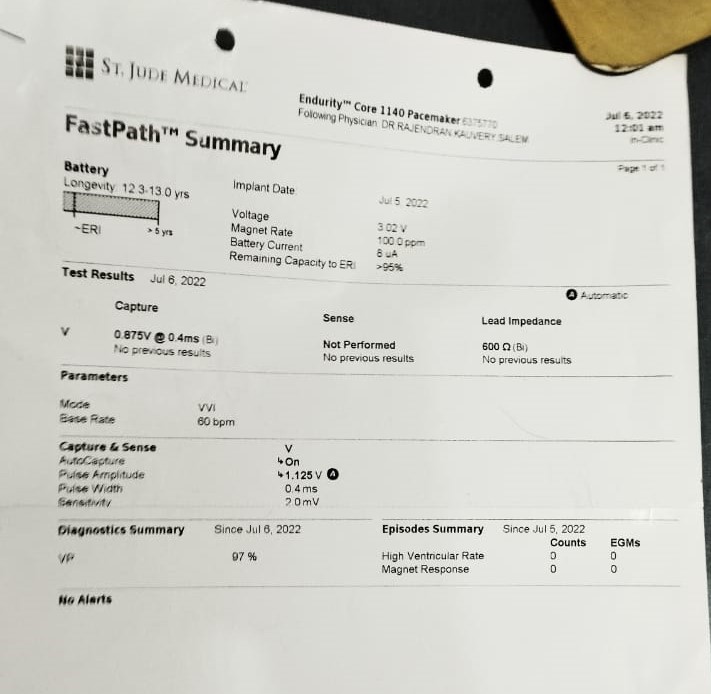 Fig. 5. PPI report sheet on 6th of August with stable Heart rate.
Fig. 5. PPI report sheet on 6th of August with stable Heart rate.
 Fig. 6. Medtronic Micra AV pacemaker is an advanced device, weight less and non-allergic to patient. Weight=1.75gm, volume-0.8cc, wireless, longevity-13yrs, safely scan a pacing system.
Fig. 6. Medtronic Micra AV pacemaker is an advanced device, weight less and non-allergic to patient. Weight=1.75gm, volume-0.8cc, wireless, longevity-13yrs, safely scan a pacing system.
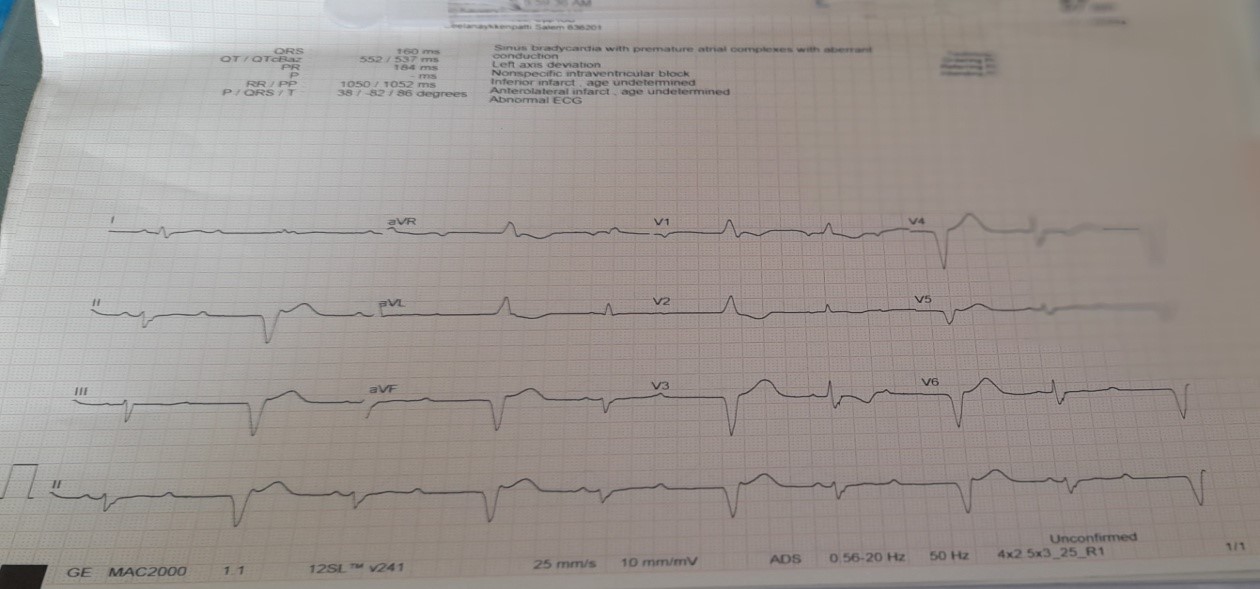 Fig. 7. ECG findings post permanent pacemaker insertion; Patient was stable with heart rate 78-80 beats/min maintained.
Fig. 7. ECG findings post permanent pacemaker insertion; Patient was stable with heart rate 78-80 beats/min maintained.
Table 1: Vital parameters
| Date | Heart Rate (beats/min) | SpO2
(%) |
BP
(mmhg) |
RR
(breath/min) |
Input/Output
(ml) |
| 1st Aug | 20 | 97 | 100/60 | 22 | 1150/1012 |
| 2nd Aug | 70 | 98 | 110/80 | 18 | 1200/1070 |
| 3rd Aug | 68 | 96 | 120/80 | 20 | 1057/1070 |
| 4th Aug | 64 | 94 | 120/70 | 18 | 1200/1300 |
| 5th Aug | 48 | 97 | 110/80 | 22 | 1250/1300 |
| 6th Aug | 60 | 96 | 120/70 | 20 | 1350/1550 |
| 7th &8th Aug | 78 | 96 | 120/90 | 18 | 1250/1500 |
Post procedure was eventful. Wound was healthy, patient improved symptomatically. He was discharged after a brief period of observation, with stable vital signs. He would however be visiting the hospital to get the device monitored over the coming months.
Nursing Care
- Monitored the vital signs HR-74b/min after PPI
- Placed the patient on a continuous cardiac monitoring for heart rate
- Obtained an ECG
- Assessed oxygenation therapy
- Checked lab investigation to ensure electrolytes are within normal limits
- Placed the patient at strict bed rest
- Auscultation done to the heart for murmur sounds
- Monitored for fluid retention- input & output maintained
- Checked the patient weight -60kg
- Put on hold any cardiac medications that can disrupt cardiac rhythm
- Educated the patient about pacemakers, microwaves and TSA security checks which can cause magnetic interference with the pacemaker
- Asked the patient to wear a medical alert bracelet
- Health education given on diet plan & restrictions, and to report any abnormal symptoms by visiting doctor.
Acknowledgment
We thank our ever-supporting management who had backed us to deliver high class services at Salem. I thank the doctors’ team for proposing the idea, and I am also indebted to the patient’s confidence reposed in us. I thank our Nursing, Cath lab team who have been very supportive in managing challenging interventions.
References
- Batra AS, et al. Fetal arrhythmias: diagnosis and management. Indian Pacing Electrophysiology J. 2019;19(3):104-9.
- Batra AS, et al. Fetal arrhythmias: diagnosis and management. Indian Pacing Electrophysiology J. 2019;19(3):104-9.
- Ellenbogen KA, et al. Clinical cardiac pacing, defibrillation, and resynchronization therapy. 5thedition. Philadelphia: WB Saunders Company; 2017.

L. Indumathi
Nurse Educator